
Access to all articles, new health classes, discounts in our store, and more!
Affirmative of the Buckley-Price Debate. Subject: Resolved, That Practically All Infected Pulpless Teeth Should Be Removed
Debate before the Odontographic Society of Chicago, October 12, 1925. Published in The Journal of the American Dental Association, December 1925.
* * *
Subject:
Resolved, that Practically All Infected Pulpless Teeth Should Be Removed
(The challenge to debate this question was issued by Dr. Buckley and promptly accepted by Dr. Price)
Dr. Johnson, Chairman, Dr. Goslee, President of the Odontographic Society, Dr. Buckley, my worthy opponent in this debate, Ladies and Gentlemen:
In accepting Dr. Buckley’s challenge to meet him in debate on the question “Resolved, that practically all infected pulpless teeth should be removed”–I have been controlled by a sense of responsibility to humanity, for I believe with all my heart that humanity needs rescuing, not from a wilful aggressor but from an incorrect interpretation which has furnished wrong fundamentals for diagnosis, prognosis and treatment.
I shall probably surprise my opponent and perhaps shock some of my audience when I confess that I hope he will win this debate by furnishing what I have not been able to find: namely, a means for sterilizing and for maintaining sterility of the infected pulpless tooth. I have searched diligently for the same for more than thirty years.
Five hundred and thirty-three years ago today, Columbus proved what the world had thought impossible–namely, that the earth was round, not flat–by the discovery of America. It certainly had seemed proof enough that anyone could see that it was flat. But Newton had discovered and propounded the newly found law of gravitation, by which objects could remain on the surface of the revolving earth. This new truth was a new sense to Columbus, and he conscientiously sailed westward, knowing he must find land or circumnavigate the earth.
Please note that some people to this day, after these centuries of circumnavigation, still believe that the earth is flat, and you have a neighbor city as a suburb of this city that still believes and teaches that the earth is flat, and there are many in the dental profession who still believe that the earth is flat.
If I could have my choice of subject this evening, it would be to discuss the new data, which relate to the cause and prevention of dental caries; for when we have solved that problem, we shall have largely solved the pulpless tooth problem by preventing it.
A new truth is a new sense simply because, with it, we can see things that we could not see before and that others cannot see who do not have that new truth; but a new truth can come only to a prepared mind. I am not here to take issue or to criticize the boasted perfection of art, engineering and mechanical skill in the practice of dentistry; but I shall take a very certain stand in opposition to the current ignorance as to where they should be utilized.
It is not in any spirit of personal criticism that I shall directly or by inference take issue with the judgment of either my distinguished opponent or the many distinguished leaders of our profession, though I shall speak frankly and plainly regarding what I believe to be serious errors of interpretation.
I believe that “practically all infected pulpless teeth should be removed” both because many of the things that we have thought we have understood are not as we have thought them to be, and also because there is a universe of new truth now available which compels a change in orientation and attitude toward the infected pulpless tooth. I refer to the newer knowledge regarding the role of focal infections in injuring immunity.
For those who may not understand my relation to this newer data, I shall perhaps be justified in stating that for more than thirty years I have maintained a private staff of workers, assisting me in the details of my investigations in my private research laboratories. (My private work is not now and never has been connected directly or indirectly with that of the American Dental Association, although for seven years I gave about half my time gratuitously to directing their work.)
These intensive studies have included not only investigations of the premises upon which former practice has been based, but also a very extensive investigation through means of blood chemistry and various other applications of biologic science to the study of the various aspects of these problems, both in human beings and in experimental animals; including more than 1,100 chemical analyses of the blood of human beings, many normal, but chiefly affected individuals, and studies of the blood of approximately an equal number of animals.
I shall accordingly spend a little time discussing why I think the old interpretations are inadequate, but shall desire to use most of my time in discussing and presenting the newer knowledge of metabolism, which so completely transcends in importance our preconceived notions that, for those who are able, because of prepared minds, it seems inevitable that it must become a new and controlling truth.
Incidentally, I find it takes six lectures of an hour and a half each to cover in even a general way these newer data. It will clearly, therefore, be entirely impossible for me adequately to present the matter in the minutes at our disposal.
My problem, therefore, will be divided into, first, a group of reasons why we cannot do what we thought we could, and, second, a group of reasons why we should not undertake to. My general outline of approach to the problem will be as follows:
Outline of Affirmative
Evidence indicates that
- The present very high death rate from degenerative diseases is due in part to unwise treatment and retention of infected pulpless teeth.
- It is so difficult as to be practically impossible to sterilize infected cementum in the mouth.
- Individuals are so very different in their susceptibility to and defense against destructive degenerative diseases as to require different consideration and treatment.
- The new evidence from blood chemistry reveals that the toxic substances from infected teeth can and do destroy the body’s normal defenses and these seriously disturb or destroy function.
With regard to the first, I shall ask you to see what Dr. Livingston Farrand had to say to the American Association for the Advancement of Science at the December meeting, 1922, at Boston, from which address Science reported as follows:
“Dr. Farrand reviewed the progress of public health work in this country and pointed out that since 1870 the average length of life has been increased by fifteen years, that marked reduction has occurred during this period in infant mortality and in mortality due to tuberculosis, typhoid, smallpox, and. many other diseases. The efforts of health workers and organizations have, however, been unable thus far to prevent increases in certain unconquered diseases, such as cancer and diseases of the heart and kidneys. The most outstanding problem at present concerns the control of the degenerative diseases of later life, an increase in mortality from these being an inevitable consequence of improvements in the control of diseases of infancy and youth.”
We can get important help from the statistical researches of the Metropolitan Life Insurance Company. Dr. Haley Fiske, president, says in the Outlook, Jan. 30, 1924: “It has been estimated that 2% of the population of the U. S., or more than 2,000,000, have organic heart disease…The annual death toll of heart disease in the U. S. is 150,000.”
Few of the students of these problems of the world have a better right to speak, because of both long years of intensive study and an unusual opportunity in the largest clinic in the world, than has Dr. Charles Mayo. He is quoted (Lancet, June 13, 1925) as stating, in a London address: “In America there had recently been a tremendous increase in heart disease and in infections, and post-mortem examination seemed to show that much of this was fundamentally due to the teeth.”
It is my personal belief that one of the strongest arguments to be brought at this time will be the death rate statistics for various communities, some of which have had for some time not only a conviction, but also a principle of practice for a number of years in a continually enlarging group of members of the dental profession, and these local communities have been quite largely influenced by the local teachings of the dental institutions furnishing the profession for these communities, and further influenced, and perhaps even more largely, by the development of study clubs, which have been taking up the pathologic, and therefore basic, rather than the technical problems of dental practice.
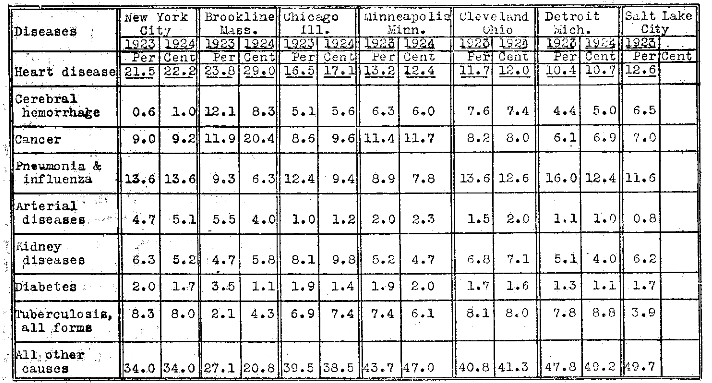
I have accordingly secured from the officers of various communities a detailed statement relative to the actual number of deaths from each of the principal causes, and have assembled these in chart form for your information. Will you please note (Table 1) that in Minneapolis, in whose state institution for the teaching of the art and science of dentistry root-filling has not been taught for six years, and where the entire community has been both directly and indirectly influenced by that advanced position, the death rate percentage of heart disease has been, in 1923, 13.1, and, in 1924, 12.4; in Iowa, which has been conspicuous for its study clubs and for men with prepared minds: 1923, 8.2, 1922, 8.1; Cleveland, 11.6, 1923, 12.0, 1924; Detroit, 10.4, 1923, 10.7, 1924; Chicago, 16.5, 1923, 17.0, 1924; New York City, 21.5, 1923, 22.2, 1924; Brookline, Mass., 23.8, 1923, 29.0, 1924.
Table 1. Principal Causes of Death From Degenerative Diseases.
I recently asked a manufacturer of dental broaches how the present sale of them compared with former sales, and his reply indicated that they were still being sold in localized districts. I have also recently communicated with the vice-president of the Ransom & Randolph Co., regarding this matter, and he has kindly given me permission to quote from his reply:
“In response to your inquiry concerning the sale of broaches and root-filling materials, in the territory covered by our various houses–Ohio, Michigan, and Indiana–there has been a very decided falling off on the sale of broaches in recent years, particularly during the past five years. As an estimate, I would say there are not more than one-third of the broaches sold at present, that there were a decade ago.”
When we realize that the annual deaths from heart disease for all of England and Wales is about 10.5 per cent of all deaths, and that more than one out of five of the funerals in New York City and Brookline follows a heart case, and one in six in Chicago, as compared with many otherwise comparable communities, we are confronted with a very grave responsibility; for just as tuberculosis has been greatly reduced as an arch slayer, so should and will heart disease be in my belief, when we come to understand and put into practice programs that will eliminate many of the contributing factors.
I cannot state how many of the cases of death in these cities were directly caused by dental infections, but I am compelled to believe that it runs into tens of thousands. The great trouble is, we do not have a conviction and tide of public sentiment. Things are taken to be what they seem to be, not for what they really are. We are, with regard to heart conditions, where as many communities were with epidemic scourges in the past, and the lines penned by Ross, as his heart was breaking in the realization of the scourge of malaria, are applicable to this today in most of our supposedly civilized communities:
“The painful faces asked, can we not cure?
We answer, No, not yet; we seek the laws.
O God, reveal thro’ all this thing obscure
The unseen, small, but million-murdering cause.”
How much dental infection does it take to ruin a heart in an individual who is susceptible, or, if it has elective localization qualities, even in an animal without special susceptibility? Figure 1 shows the heart of a rabbit that died from endocarditis and reveals a vegetation an inch long produced by injecting into the rabbit the practically clear washings of two crushed teeth that had been extracted from a man, 26 years of age, suffering with acute endocarditis. The quantity of organisms was calculated by a counting method and found to be less than a millionth part of a gram.

Fig. 1. Valvular vegetation in heart of rabbit which died of endocarditis after being inoculated with washings of two crushed teeth from a patient suffering from acute endocarditis.
In another case, cultures from the tooth of a boy suffering from acute endocarditis and rheumatism were inoculated into thirty rabbits. Twenty-eight of the thirty rabbits, or 93 per cent, developed acute heart involvement, and thirty of the thirty, or 100 per cent, developed acute rheumatism. This boy died a few months later. He, as we will see, was practically doomed before he was born, for he had by inheritance a marked susceptibility for heart involvement, and he was born in an age and in a community that did not yet have sufficient new truth to protect him against his preventable but impending doom. It would be fortunate if an entire hour could be given to the citing of such specific heart cases.
Similarly, we should note the relation of certain types of arthritis to dental infections. Sir William Willcox and Dr. Beddard of England state: “Ninety per cent of the cases of non-specific infective arthritis are due to infections arising from the teeth.” And regarding the prevalence of this type, Ely of San Francisco states: “In the orthopedic clinic at Stanford it is by far the most frequent disease with which we have to deal. Established always with the roentgen rays, its diagnosis comprises more than one-tenth of the diagnoses in our clinic.”
Similarly, we should review, if time permitted, certain affections of eyes, kidneys, nervous system, etc.
Second: It is so difficult as to be practically impossible to sterilize infected cementum in the mouth. (see charts, pp. 289 and 291 in Brooks and Price, reference 1)
Our second division presumes that infected teeth can be sterilized. After more than thirty years of investigation on this problem, I am compelled to state my belief that the number of instances (and I shall present evidence supporting them) in which infected teeth have been completely sterilized would be less than five in 100, to say nothing of the difficulty of keeping them sterile.
At this point, I wish in all kindness, but in complete frankness, to state that I am not in accord with advertising propaganda that would make these procedures seem easy and safe for the members of the dental profession, as I will show that I cannot, by any means that has been known to me, succeed in sterilizing infected cementum by treating it through the dentin. I know full well that there are many men perfectly convinced in their own minds that they can do this thing.
Dec. 17, 1922, I received a letter from Dr. Davis, from the office of the director of the Caulk Dental Research Institute, Milford, Del., in which he stated:
“In so far as I have been able to test out any materials I have not been able as yet to sterilize the cementum within the mouth, even though I applied them sufficiently strong to destroy the surrounding tissues.”
I quote herewith Dr. Davis’ telegram dated Oct. 8, 1925, authorizing me to use this information and giving the results of his further studies:
“You may quote from my letter as requested. No evidence as yet to change that view. Open to conviction. Hope for day when therapeutics will destroy deeply embedded anaerobic infections. Till then physicians and dentists must resort to surgery. Still experimenting.”
The infected pulpless tooth, with which we are starting as a premise, is an infected sequestrum so far as all those structures are concerned which are infected. We are immediately then confronted with the problem as to whether or not we can sterilize it and whether or not it will stay sterile. While I could readily take the entire time for this and many others of the single problems involved, I can present only about one or two slides as typical of each problem.
When sterile J. & J. absorbent points carrying the medicament were placed in infected teeth, which are the subject of this debate, and the points were removed after periods of time, five, twenty-four, and forty-eight hours, and cut into sections, 1, 2, 3 and 4, numbering from the root apex up, all but one were infected in forty-eight hours, all but three in twenty-four hours, and only four had some efficiency if tested within five hours. In a mouth in which periapical exudate was present and the root tip was immersed in infected culture medium and the disinfectant placed in the pulp canal, practically all dressings were infected in each five, twenty-four and forty-eight hours.
When we remember that a single rooted tooth has approximately 3 miles of closed canals when we place the dentinal tubuli on end in series, we get some conception of the difficulty of sterilizing even the dentin. In more than 95 per cent of cases in which we have placed a medicament in a canal on a dressing, when the tooth had periapical involvement, we have in forty-eight hours been able to grow cultures from the dressing that was placed in the tooth, regardless of the medicament that was placed on the dressing.
In the foregoing and many other investigations, which have been reported in detail,1 it is demonstrated that it is extremely difficult to sterilize infected dentin. Even the placing of small pieces of infected dentin in dilutions of solution of formaldehyde U. S. P. and other medicaments, such as can be used in the mouth, takes considerable time.
The problem becomes very different when it comes to the matter of sterilizing infected cementum by the treatment of infected dentin. For years, I have been not only searching myself for a medicament competent to sterilize tooth structures in the mouth, for I have earnestly wished that this could be accomplished, but also I have been announcing in connection with lectures, as I have gone about the country, a reward of $500 for a means that would accomplish this. After years of study of this problem, I feel sure that I cannot do this by any means that I can safely use in the mouth, and I question very much whether many people have ever spent so much effort in trying to do so.
We have, for example, allowed fuming concentrated solution of formaldehyd to trickle through the pulp canal of a tooth which had the infected cementum protected with a rubber dam above and below, until 10 c.c. had passed through, and the cementum was still infected; for the neutralized tooth was planted beneath the skin of a rabbit under surgical conditions, and an abscess developed containing pure culture of streptococci.
Similarly, we have used silver nitrate neutralized with solution of formaldehyd, giving treatment much more thorough and extreme than could be given in the mouth. The animal under whose skin this tooth was planted died from a large abscess. Figure 2 shows the dissection of the animal and the diplococci which grew out of that tooth after such severe treatment.
Fig. 2. Abscess produced in rabbit from supposedly sterilized tooth; also diplococci which grew from same.
We can visualize the structure of the dentinocemental boundary by thinking of the details involved in the formation of a tooth. The two formative organs, building toward each other, throw down at first a common continuous wall, which is in effect like a bottle or flask, the opening to which is at the root apex. The dentin is built onto the inner side of the bottle and the cementum and enamel on the outer side of the bottle. The dentin has its interior network of channels provided by the retreating odontoblasts as dentinal tubuli formed by the protoplasmic cellular extensions from the dentin. The cementum is built around the cementoblasts, which form the lacunae of the cementum, and these included cells are connected with other cells by protoplasmic structures which constitute the canaliculi.
The impervious nature of this common boundary, except for the mouths of the bottle, to which we shall compare the apical and other foramina, through which blood vessels pass, has been abundantly demonstrated by many workers. Silver nitrate, for example, placed in the interior of a tooth stains the dentin but does not stain the cementum. Similarly, silver nitrate placed on the exterior of a tooth stains the cementum but does not stain the dentin. The disinfectant, therefore, that is placed in the dentin of a tooth must, in order that it may reach organisms in canaliculi and lacunae of the cementum, pass through the single or multiple foramina, proceed along the external surface of the tooth to the canaliculi, and then pass inward through hairlike canals to the lacunae and there attack the relatively extensive infection in the lacunae. If, as has been abundantly demonstrated, all the disinfectant that can be put on a root-canal dressing placed in an infected pulp canal of a tooth which has periapical involvement cannot even keep the dressing sterile, how can it sterilize the periapical area and send a concentrated medicament back into the canaliculi to sterilize the lacunae?
The entire problem of whether or not infected pulpless teeth should be extracted or may be treated should perhaps be settled right on this fundamental premise; for if this cannot be done, there is no basis for argument. In this connection, I will state that we have passed a concentrated solution of compound A of Table 4 through a pulp chamber from Saturday until Monday without destroying the organisms in the cementum of the tooth being tested.
We come now to the question as to whether or not, even granting for the sake of argument that a tooth can readily be sterilized in the mouth, which I do not grant except for argument, a root-filling material can block infection from it. I have previously published2 extended investigations to determine whether or not it is feasible so to fill the root canals in sterile teeth that infection cannot reenter the tooth structure.
Figure 3 shows a series of such tests in which freshly extracted, autoclaved teeth were root-filled by the various methods and then placed in infected culture mediums for definite periods, after which they were cultured in the various structures, with the alarming result that the great majority of the teeth had infection in the dentin of the tooth and many of them in the root filling material itself in two weeks.
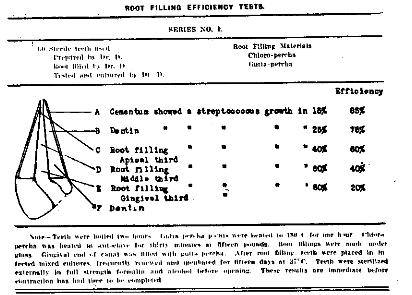
Fig. 3. Limited ability of root fillings to block out streptococcal infection from tooth structures.
On the presumption that we were not so skilful in the art as others, I selected five dentists with national reputations and submitted to them teeth which, after being extracted, had been placed in plaster-of-Paris blocks and the blocks autoclaved at 30 pounds for half an hour. These blocks were sent to the operators for placing root-fillings by their methods. On receipt of the blocks the teeth were placed in infected culture mediums for two weeks and then cultured in their various structures, and it is pathetic to record that only two teeth in the lot did not grow cultures from root-filling or dentin (Table 2.) I am sure that the average dental operations of the best operators of the country would not make so good a showing as this, even assuming what I believe to be nearly impossible, that they could sterilize the tooth.
Table 2. Tests of Efficiency of Root Fillings Placed In Sterile Teeth by Five Dentists of Reputation.*
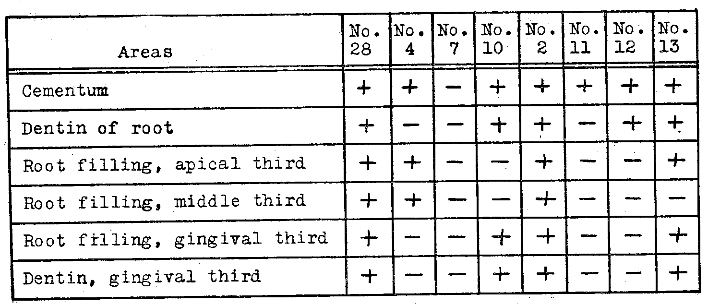
*Freshly extracted teeth were autoclaved in moist plaster blocks and submitted in sterile containers for root-filling. On receipt, they were placed in infected culture mediums for two weeks. +, positive growth.
In connection with the ability of an operator to place a safe root-filling, I wish to present in Figure 4 a series of root-filled teeth with the following history. At an important convention, during the discussion of root-fillings an operator made the statement that he believed that he could fill 95 per cent of molar teeth perfectly to the ends of the roots. He was challenged by a confrére from another part of the country, and a bet was made, the outcome of which was that I was to be umpire and furnish No. 1 with a group of molar teeth invested in plaster-of-Paris blocks, the teeth to be returned to me for examination.
The result was most pathetic, for only a small percentage of the roots were filled to the end, but many roots were filled through the sides and some of them for a considerable distance. His explanation of the latter fact was that had the patient, instead of the plaster-of-Paris, been behind the tooth, the pain suffered by the patient would have prevented him from going so far.
In this connection, how many dentists have been filling four canals in the majority of upper first molars? And yet Orton has shown that 75 per cent of upper first molars have four root-canals. (Walter Hess in Hess and Zürcher says [p. 34]: A division of the mesio-buccal canal I could find in only 53 per cent.–Editor.)
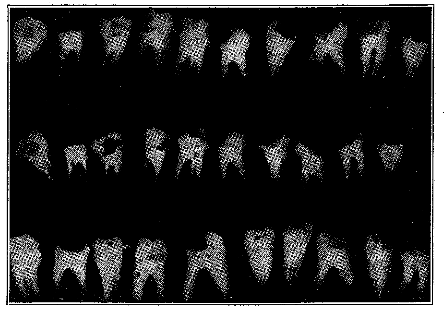
Fig. 4. Tragic failure of an expert who had claimed he could fill 95 per cent of molar roots perfectly. Not 5 per cent were efficiently filled; many were filled through the side and many canals were not filled (as usual).
Let us take a practical case, studied in another way. Figure 5 shows three views of two lower molar teeth. In A, we have the condition beneath a gold crown where there was a suspicion that the pulp was degenerating. The pulp was removed and the tooth root filled in our office by an expert, who I believe has skill that is not surpassed. B shows the tooth after root-filling, and C, the tooth seventeen months later. The patient promised to permit them to be extracted.
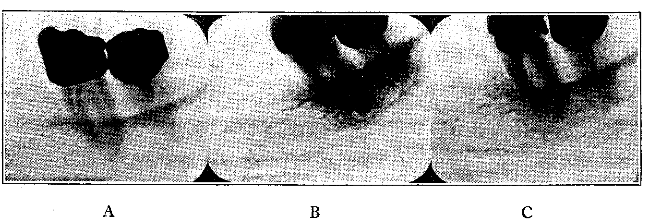
Fig. 5. The appearance of two teeth: A, before and B, after root-filling; and C, seventeen months later. (See Table 3.)
On removal, the mesial root of the second molar (showing two root-fillings) was placed under the skin of one rabbit and the distal root under the skin of another (Table 3). These teeth were first washed thoroughly with physiologic sodium chlorid solution and the placing was done with surgical asepsis. Purulent infection developed about each root but much more rapidly about the mesial root than the distal. The mesial root killed four rabbits in succession in an average of six days, with an average loss in weight of 20 per cent. The distal root killed two rabbits in thirty days, with an average loss in weight of 31 per cent.
Table 3. Results of Implantation of Teeth Under Skin of Rabbits.*
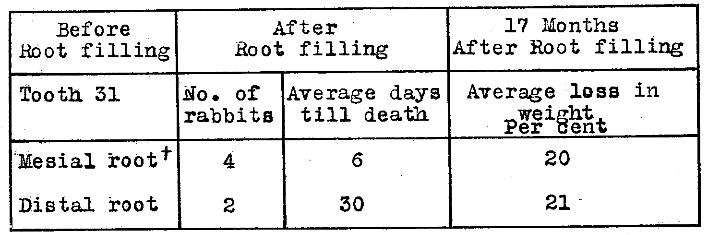
*These teeth are shown in Figure 5.
†The mesial root was then boiled and again implanted. This rabbit gained 21 per cent in six weeks.
The mesial root was then boiled and placed under the skin of a rabbit, and the animal in the next month and a half gained 21 per cent, and was apparently normal. If rabbits could speak, I am sure they would advise boiling as the means for sterilizing infected pulpless teeth.
This whole problem of root sterilization presumes that, when a tooth is made uninhabitable, it will remain so. This, however, does not take into account those qualities which are involved in the adaptability of organisms to their environment. (Tables 4 and 5.)
I will now take up a matter which has great importance for the members of the dental profession; namely, the question of bacterial accommodation. I have previously shown3 that streptococci have a quality which is characteristic of many other types of organisms of being able to adapt themselves to an unfavorable environment in a way that is most striking. For example: A certain strain of streptococcus requires a dilution of 1 to 10,240 in order to begin growth, but with increase in the concentration in medicament came gradually to grow in from 1 to 320. This has been reported for Spirochaeta pallida and for the gonococcus. Varieties in the method of culturing produce quite dissimilar results.
The blood fluids bathing an infected tooth contain buffers of remarkable efficiency for neutralizing chemicals. This quality is an essential for life and characterizes all tissues and fluids. One of the culture mediums used was dextrose brain broth which is particularly favorable for the growth of the strains of streptococci found in dental foci.
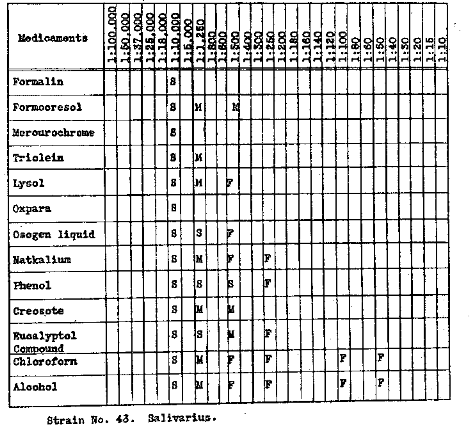
In Table 4 will be seen the result of using formalin, formocresol, mercurochrome, triolin, lysol, oxpara, compound A (said to contain magnesium chlorid, potassium iodohydrargyrate and water) for two groups, and compound A mixed with compound B, the latter said to contain magnesium oxid, barium sulphate, mercurous chlorid and dithymol diiodid. In that same column, natkalium, phenol, creosote, eucalyptol compound, chloroform, alcohol, sodium cacodylate, and N-hexylresorcinol are listed. Strain 43 is shown by two methods of culture, one in which all dilutions were inoculated at once, and the lowest showing growth was recorded and the other transplants made daily and left two days in each dilution. It will be noted that in many of these substances there was a decrease in the dilutions at which growth was possible, the differences in some cases being as great as 1 to 10,000 for all dilutions not made at once and from 1 to 400 for the daily transplants. You will note particularly the high efficiency of the last drug mentioned, the one recently discussed. Time does not permit of a complete analysis of the fund of information revealed in the chart, which will be readily disclosed to those who make the study.
Table 4. Bacterial Accommodation: Acquired Tolerance of Streptococci (From Dental Foci) to Various Medicaments
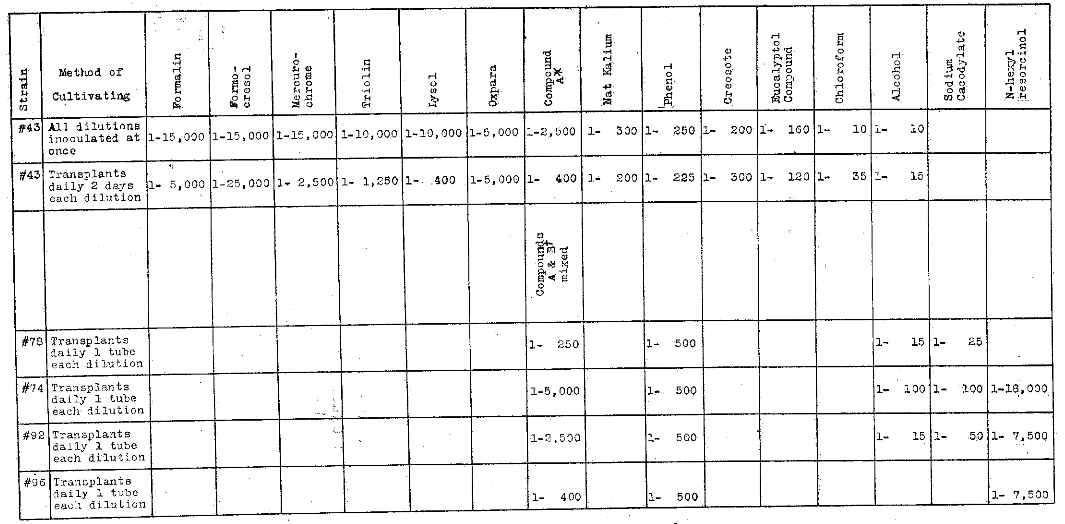
*Compound A is said to contain magnesium chlorid, potassium iodohydrargyrate and water. †Compound B is said to contain magnesium oxid, barium sulphate, mercurous chlorid and dithymol diiodid.
The question of the method of inoculation is of particular importance since, in the tooth in situ, the organisms will find various gradations of conditions which can make their advancement along the lines and in the zones most favorable, owing to the marked neutralizing effect of the body fluids, particularly varied in the infected tooth.
The bacterial accommodation is rapidly diminished. In order to throw light on this phase of the question, we have made inoculations by many different methods, eleven of which are shown in Table 5, which reveals very important new data. In general, the method of rapid transplanting in dextrose brain broth daily gave the most marked changes when compound A or a mixture of A and B was used.
Table 5. Acquired Tolerance or Bacterial Accommodation of Streptococci Under Various Experimental Conditions to Compound A* and Compound B†.
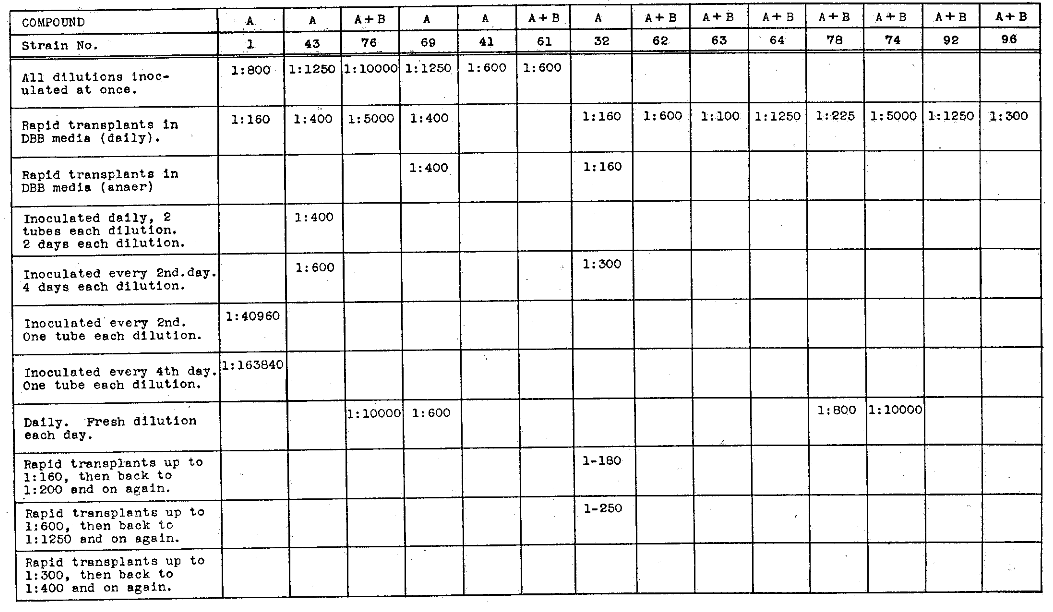
*Said to contain magnesium chlorid, potassium iodohydrargyrate and water.
†Said to contain magnesium oxid, barium sulphate, mercurous chlorid and dithymol diiodid.
Another important matter has come out of researches on this problem; namely, that there is a great difference in strains of streptococcus. For example, in Table 5 when all strains were inoculated at once, strain 1 grew in 1 to 800 of compound A; strain 43, 1 to 1,250 of A; strain 76 required a dilution of 1 to 10,000 to grow in a mixture of A and B, while strain 61 grew in this mixture in 1 to 600; strain 41 grew in from 1 to 600 A; while strain 69 grew required a dilution of 1 to 1,250 of A. By the rapid daily transplanting method in dextrose brain broth two strains 1 and 32 will be seen growing in from 1 to 160 of A and strain 63 grew in 1 to 100 of a mixture of A and B; strain 96 in from 1 to 300 of A and B; while strain 74 did not grow within this time of experiment lower than in 1 to 5,000 of a mixture of A and B. Strain 78 grew in this mixture in 1 to 225. A daily fresh dilution of a mixture of A and B with strain 78 grew in 1 to 800; strain 76 as well grew in a dilution of from 1 to 10,000 of this mixture, which emphasizes the importance of fresh medicaments in infected teeth. The direct application of this information would be to treat the infected teeth daily, indefinitely.
The total amount of medicaments that can be placed in an infected tooth being too small even to destroy the infection of the tooth readily, as I have shown, we see how complicated the problem becomes of having this medicament maintain concentration in the presence of the body buffers or neutralizing agents sufficiently to continue to destroy streptococci which pass through the circulatory system in swarms each time we catch cold and readily reach the apex of the teeth from gingival pockets about the teeth.
Another important phase of our newer data relates to bacterial mutations under the conditions provided in a medicated tooth. When Rosenow first presented his data indicating mutations, the proposition was not kindly received by most of the leaders of bacteriologic teaching, and I think we may say it is not by some of them today. It is, however, significant that many of the leaders of today are presenting evidence supporting the correctness of his position. To illustrate, Libman, in a paper read before the Michigan State Medical Society, Sept. 11, 1924, states:
“The aerobic streptococci are divided into hemolytic, nonhemolytic, or anhemolytic (so-called Streptococcus viridans) and the Streptococcus mucosus-capsulatus. The opinion which Dr. Celler and I have had for many years that the anhemolytic streptococci represent transition forms between pneumococci and hemolytic streptococci is now receiving much support.”
You will note that Dr. Libman suggests that he and Dr. Celler believe that the anhemolytic streptococci, or viridans group, represent transition forms between pneumococci and hemolytic streptococci. The term viridans is the group name of the nonhemolyzing streptococci which produce a narrow green zone when grown on blood agar.
In Table 6, I have shown nine different strains of streptococci which are frequently found in the mouth, and some of them occasionally, and some frequently, in dental infections. All of the first six, are viridans: namely, fecalis, ignavius, salivarius, in frequens, mitis, nonhemolyticus I, nonhemolyticus III. The last three are not viridans because they hemolyze and do not produce the typical green zone: namely, hemolyticus I, subacidus, pyogenes. (These are called hemolytic strains.)
Table 6. Relative Prevalence of Different Strains of Streptococci
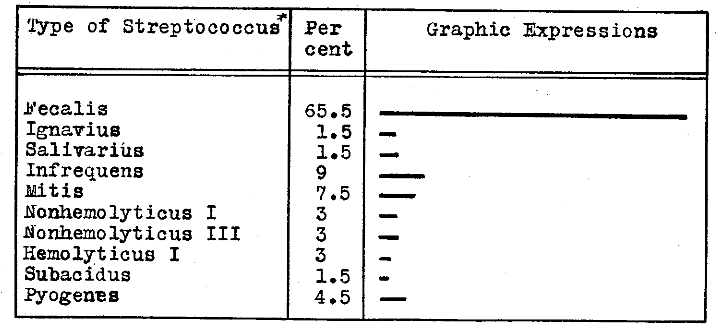
*Streptococcus viridans is the group name of nonhemolyzing streptococci producing a narrow green zone when grown on blood agar. The first six are viridans. Note that 65 per cent of strains recovered in animals were fecalis.
You will remember that these are different strains of streptococci and in general look alike when seen under the microscope. They are differentiated by their behavior in culture mediums, particularly their ability to ferment certain sugars.
In Table 6, I have shown the relative frequency of these various organisms as they have appeared in the lesions produced or reproduced in animals inoculated with cultures from the teeth of ill patients, and you will kindly note that 65.5 per cent of the strains are the fecalis group, only 1.5 per cent salivarius, and only 7.5 per cent mitus, and the others vary but are all small amounts.
With regard to these various strains, it is very important to note that the usual relatively harmless strain found in the mouth is a salivarius. It is in babies’ mouths soon after birth and can be found in most mouths throughout life, and more frequently than other strains in that simple environment. It therefore is most frequently available for the inoculation of dentin and pulps and through the pulp chambers to the tooth structures and apical areas.
Please keep in mind that this is not the strain that we generally found in pure culture in the hearts, joints and other diseased organs of animals inoculated with the cultures from the teeth which had been extracted from individuals suffering from acute lesions, which the animals frequently reproduced. As stated, the strain found in 65 per cent of the cases of a series taken in succession was fecalis.
The effect of various medicaments on changing in a test tube the type or strain of the streptococcus in question was interesting. Strain 78, when recovered from the tooth, was a mitus. In sodium cacodylate, it changed to equinus, then to ignavius, then back to mitus, then to nonhemolyticus III. In alcohol it changed to nonhemolyticus III. In compound A, it changed to nonhemolyticus I. In phenol, it remained a mitus.
Strain 43 (Table 7) was a salivarious to start with and changed in many of the medicaments to a mitus, and in many changed to a fecalis, when it came to grow in an increased concentration of an irritant. Is it not clear that, by submitting the organism to an irritant, we have made it more virulent and more dangerous? Similarly, the behavior of the various strains will be followed through on that chart, which is most illuminating.
Table 7. Bacterial Mutations which Have Developed in the Presence of Irritants.*
*All started as salivarius. Many changed first to mitis and then to fecalis, with an increase in disease-producing power.
Remember a new truth is a new sense because with it we can see things that we could not see before, and this new truth certainly demands that we shall look on a treated tooth in an entirely different light from that in which we have in the past, for not only do we have great difficulty, amounting practically to an impossibility, in completely sterilizing tooth structure, but also our efforts may result in the development of a more virulent organism if we have not exterminated the last one. That, however, is not all the story; for, even though we have sterilized the tooth, it can with a dissipation of its medicaments become reinfected from the blood stream and other sources and will then be the right kind of an incubator to develop a virulent strain.
Haden has shown by a method of culturing which is designed to show the colonies in a special agar medium that 54 per cent of 490 pulpless teeth which were roentgenographically negative grew out colonies, and, under the same procedure, 70 per cent of 425 which were roentgenographically positive. Will you note, please, the small difference whether the teeth were negative or positive roentgenographically? His work has also added much to the literature, demonstrating that the roentgenographically negative tooth is by no means evidence of absence of infection. (It is not at all probable, however, that his alkaline culture medium grew out all the strains present, for many are not so facultative; they require an acid medium.)
Rosenow and Meisser, by taking the cultures from patients suffering from stone in the kidney, were able to produce stone in the kidney in dogs by simply placing those cultures in the pulp canals of devitalized teeth and permitting them to continue to grow there. In spite of the normal defense of the animal’s body, a large percentage of the animals had their defense broken, and developed kidney stones; and, further, when teeth were root filled in a sterile manner in normal dogs, they tended to remain sterile for a period but soon became infected if some other tooth or teeth of that animal were filled in an unsterile manner: that is, purposely inoculated. In other words, there was evidence that the infection passed through the supporting medium and the circulation from the infected pulpless tooth to the non-infected pulpless tooth, with the result that the latter became an infected pulpless tooth. There is much evidence that just this thing happens in humans.
Third: Individuals are so very different in their susceptibility to and defense against destructive degenerative diseases as to require different consideration and treatment.
Dental practice in the past has largely looked on individuals as being sufficiently similar to be comparable with regard to the dental program that may be indicated for any given dental condition. That some individuals are more susceptible to heart or kidney or joint involvements than are the majority is a fact so abundantly demonstrated in every community that we all have been talking about this and that disease running in this and that family. What we have been seeing is that, by inheritance, there is a lowered resistance for that disease in that family. This should directly influence, and when this new truth has become a new sense in our profession, will largely determine what operations may and what operations may not be done for particular individuals.
We are also all familiar with the common expression that a draft on the neck, for example, or getting wet, caused rheumatism, or stiff neck, or what not. We have not appreciated the sensitiveness of our bodies to overloads which depress either local or general defense; and yet we are all familiar with the fact that certain affections express themselves when the individual is attacked with an acute or chronic illness. What I wish you to see is that these factors, both of inherited susceptibility and of overload, may decide whether or not the infected tooth will produce visible injurious expression in another part of the body.
Table 8, from the Lancet, Sept. 27, 1924, presents a report of Drs. Eason, Smith and Buchanan that, in a given family with twenty-eight members, sixteen have developed nephritis, and in their text, they discuss the relationship of the dental infections to the development of these lesions. In the light of our newer knowledge, members of that family should have special consideration regarding their dental care, keeping in mind this weakness in the wall of normal defense. In my own practice, our families are routinely studied, charted and classified in such a way that we often know before children are born where the inherited weak link in the chain might be expected to be, and such individuals have a program adapted and controlled by that fundamental truth.
Table 8. Genealogical Tree (Hurst)*
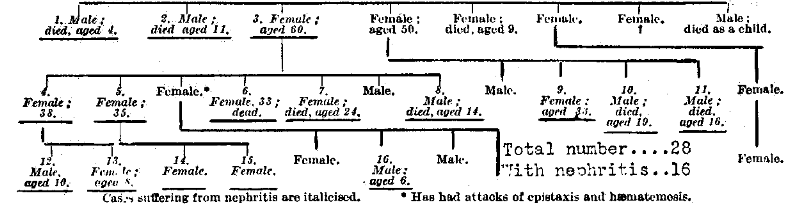
*Influence of inheritance on susceptibility to nephritis. In this family of twenty-eight, sixteen developed nephritis; hence, their increased danger from dental infections in the presence of systemic overloads.
This is more clearly demonstrated in Table 9, which shows the result of taking forty individuals, ten with joint involvement, ten with heart involvement, ten with nervous system involvement, and ten with internal organ involvement, and studying the other members of the family, approximately sixteen people for each of the ten families. When we compare the expressions of these lesions in members of the family other than the individuals studied, we find that, in the group where all ten individuals had rheumatism, the other members of that family, approximately 160 in each group, had fifty-nine instances of rheumatism, as compared with twenty-four, fifteen and thirteen in the other three groups. For the heart group, the other members of the family had fifty-seven cases, as compared with seven, nine and nine; nervous system group, 142, as compared with nineteen, twenty-five and thirty; internal organ group, ninety, as compared with nineteen, thirty and twenty-eight.
Table 9. Dominance of Special Tissue Lesion in Both Patients and Families (Ten).
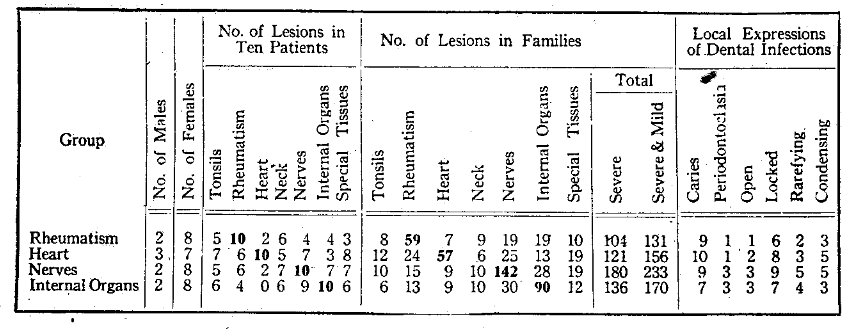
Type of susceptibility–inherited.
While the presence of an affection in a parent or ancestor might be argued to have contributed to the development of the lesion in the offspring, it cannot be so argued in these instances since the child could not influence its ancestry. On the basis of susceptibility to the rheumatic group affections, we can, as I have shown (Table 10) divide all people into three groups, absent, acquired and inherited susceptibility. The inherited group we divide into four subgroups, one side mild, two sides mild, one side strong and two sides strong.
Table 10. Relation of Periodontoclasia to Susceptibility to Rheumatic Group Lesions. (Fifteen Typical Families in Each Group. Group Two).
On this basis, it will be found that, in fifteen families with an average of sixteen people each, the severe rheumatic group lesions in the fifteen families (or an average of 240 people) will be in the absent group sixteen cases, the acquired group sixty-three, inherited one side mild 144, inherited two sides mild 227, inherited one side strong 258, inherited two sides strong 483, where, when we include the severe and mild lesions, the severe being those that will kill or incapacitate and the mild those that will cause to suffer but not seriously injure, the figures are 31, 96, 201, 308, 338, 754. In other words, the individuals in the latter groups have a potential possibility for injury from an adequate source of infection, of which dental infections are the most common and most severe, from twenty to thirty times as great as the individuals in the first group.
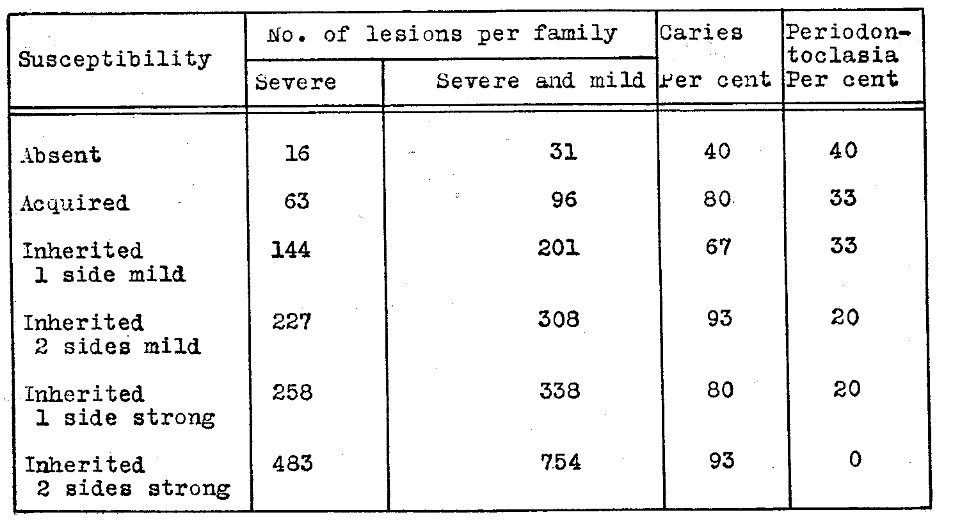
On the basis of dental pathologic processes in relation to local irritants, such as infection, we can again divide all people into three groups: first, those with large areas of rarefaction, as illustrated in A and B of Figure 6; second, those with large areas surrounded by zones of much condensation, C and D; and, third, those who even with much infection, such as all the infection of an infected pulp, have very little rarefaction about the root end, as shown in E and F, and often much condensation, or all the bones are dense.
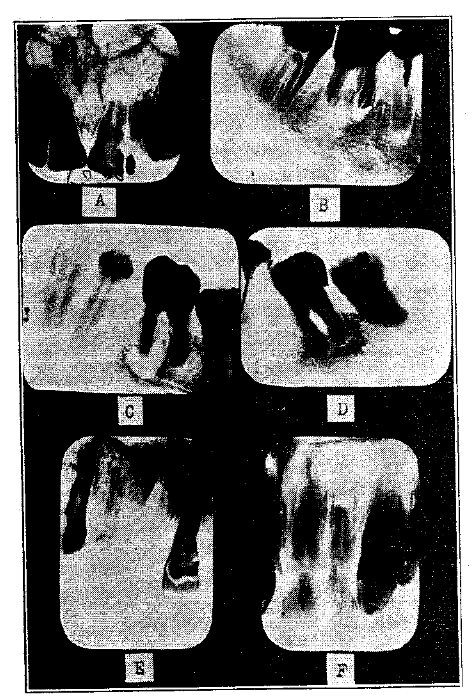
Fig. 6. Classification of individuals into three groups on the basis of the type of bone change, with a given dental infection.
When we relate these two factors, we find a typical illustration (Group I, Fig. 7) of a man, 52 years of age, in 1917, now over 60, a member of a large family and practically never sick a day in his life. His only trouble is an eye involvement; he cannot read late as he used to, unaided by glasses, and roentgenograms reveal very extensive decalcification. It is now demonstrated beyond the possibility of question that the individuals who developed a large zone of rarefaction did so at the time when they were able to produce decalcification as a part of a defensive mechanism, and large areas are therefore diagnostic that the patient has had in the past, and possibly up to the present, a high defense.
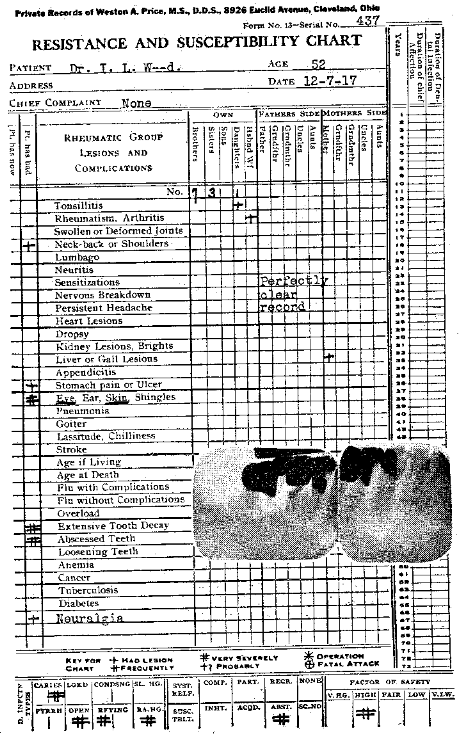
Fig. 7. Group I, by each of two methods of classification: absent; susceptibility of patient and family, and marked decalcification.
Group II (Fig. 8) relates the individuals with the broken susceptibility, due to overload, with the type of dental pathologic process, the condensing osteitis around the rarefying. In this case, a woman, 22 years of age, who had had influenza, with a nervous breakdown, had experienced a rapid recovery after the removal of her dental infections. Note the zone of calcification around the rarefaction, and also note the effect of overload on an individual who had normally a high defense.
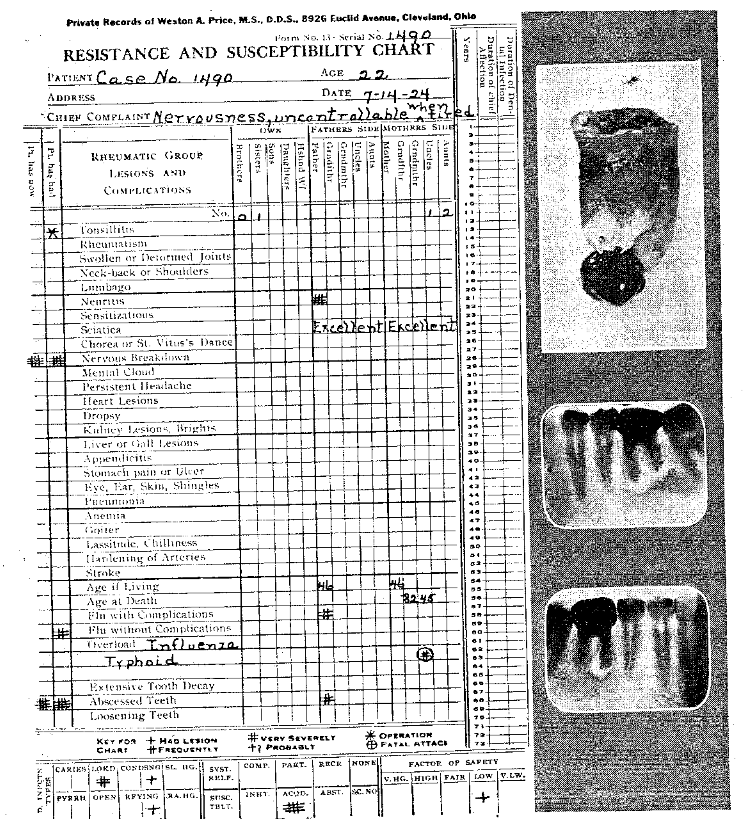
Fig. 8. Group II, by each of two methods of classification: acquired; susceptibility with overload, and zone of condensation about zone of rarefaction.
Group III (Fig. 9) is represented by the case of a woman, 24 years of age, who was ill of heart trouble and rheumatism, and whose father and mother both died from heart trouble. There were nine cases of rheumatism and seven of heart disease in the family. The patient was doomed before she was born unless she chanced to live in a community where this new truth had become a new sense: namely, that by keeping free from a source of streptococcal infection she might still, in spite of her handicap, have a relatively comfortable life, provided she kept her overloads reduced. With the removal of the sources of dental infection, she returned to her work, and she has not yet had a second break.
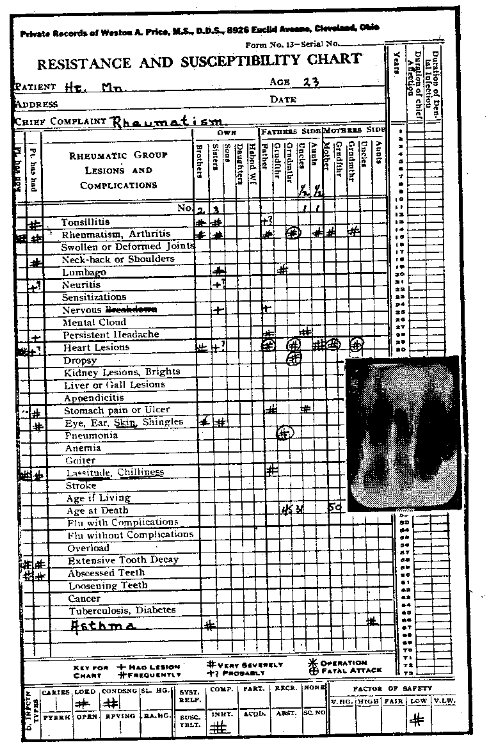
Fig. 9. Group III, by each of methods of classification: inherited susceptibility of individual and of family; relatively slight bone change about tooth with putrescent pulp.
When, now, we relate these important factors to the type of disease that develops in an individual, we find, as shown in Table 11, that those individuals in the inherited susceptibility group have a lower than normal blood active or ionic calcium, and the bactericidal efficiency of their blood low. They are the group in whom dental pathologic processes are expressed with little rarefaction, and often with considerable condensing osteitis, and the group which suffer from heart, proliferative arthritis, acute rheumatism, caries, kidney involvement, stroke and nervous breakdown.
Table 11. Relation of Calcification and Decalcification to Type of Systemic Disease
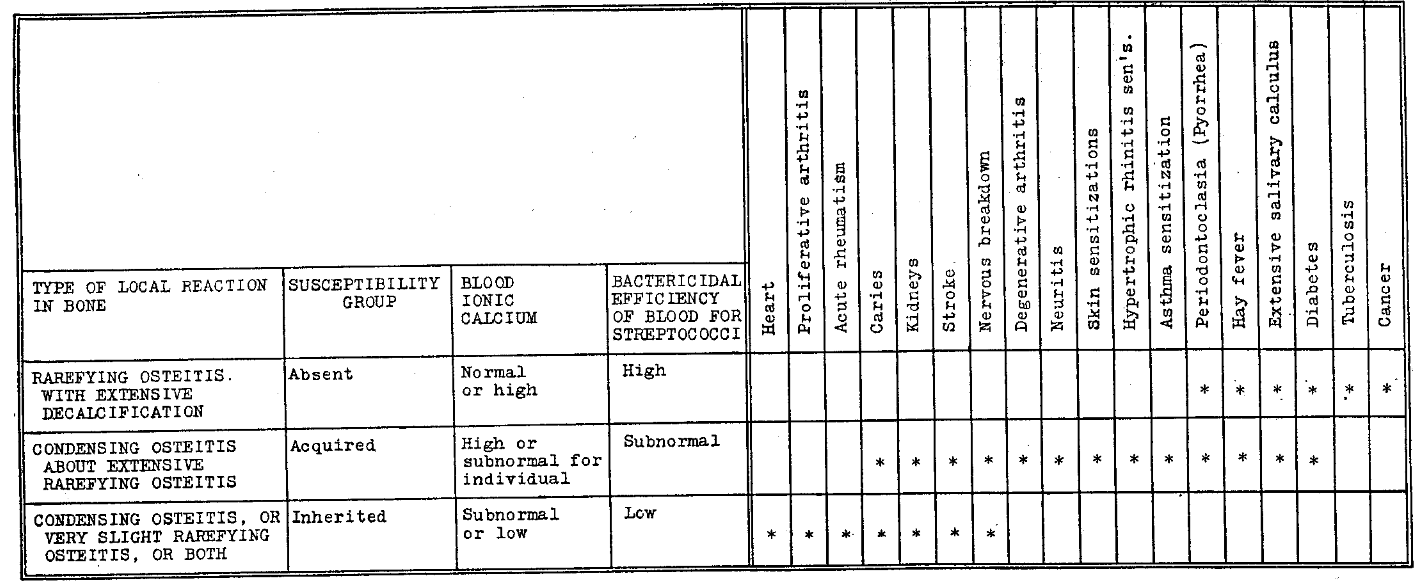
The second group from the bottom, or middle group, with the condensing osteitis about an extensive rarefying osteitis as their dental characteristic, have the acquired susceptibility to the rheumatic group lesions, usually because of overloads: pregnancy, influenza or such affection. Their blood ionic calcium, which is now low, was formerly high. The bactericidal efficiency of the blood is now low, and they of that group now suffer acutely from dental caries. They may have kidney involvement or stroke, nervous breakdown, degenerative arthritis (not proliferative), neuritis, the various sensitizations of the skin or respiratory tract, hay fever, etc.
The people in the upper group with the marked rarefying osteitis without condensing osteitis about it as their dental characteristic have complete absence of susceptibility to the rheumatic group lesions; the blood ionic calcium is normally high; and the bactericidal efficiency of their blood for streptococci is high. This group, while not suffering from the rheumatic types of degenerative diseases, furnishes the individuals who may have the sensitizations, hay fever, asthma, etc., and furnish almost all those with diabetes, tuberculosis, cancer and many of the severe anemias.
Table 12 presents findings in a group of 100 cases studied intensively with regard to the development of cancer, tuberculosis, diabetes, anemia and stroke, in which it will be noted that the percentage of these lesions is low in those individuals who have been suffering from the severe rheumatic group affections, and is high in those who have a history of being free from these affections during their lifetime.
Table 12. Findings in Study of 100 Consecutive Families*
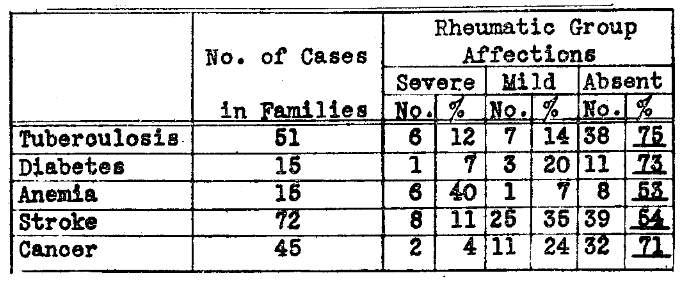
*Study of association of nonrheumatic group affections with presence or absence of rheumatic group susceptibilities.
Time does not permit my introducing a quantity of evidence that I should wish to, demonstrating the calcium levels of the individuals of these three groups. I have recently presented these and many related data on the interpretation of calcium in a paper before the American Dental Association, entitled “Newer Knowledge of Calcium Metabolism in Health and Disease, with Special Consideration of Calcification and Decalcification Processes, Including Focal Infection Phenomena,” which will be published in The Journal of the American Dental Association in due time. (It should be noted, that Dr. Haven Emerson has recently shown that diabetes has increased in New York City 1,426 per cent since 1866, and that this increase comes almost entirely in the individuals 45 years of age and over.)
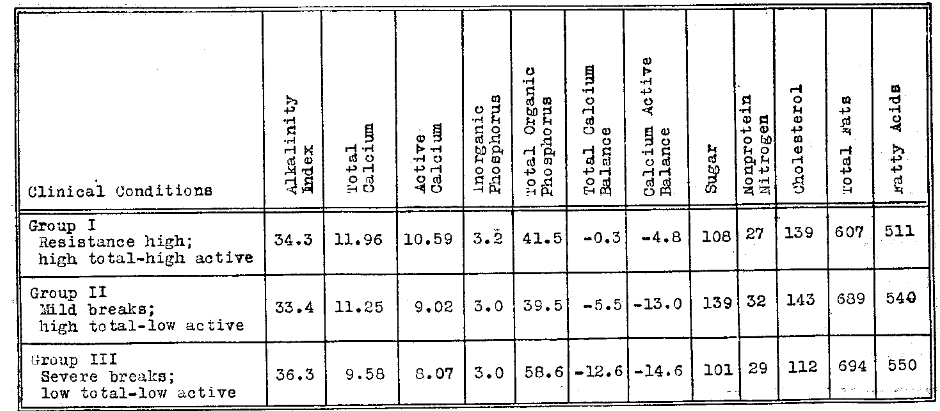
Table 13 is a summary made from these charts, showing the average total and active calciums of the individuals in each of the three groups, and it will be noted that both total and active calcium tends to be high in the group with a high defense characteristic of those classified under absent susceptibility; that in those with a broken defense, or an acquired susceptibility, the total calcium tends to be high, though when the condition is severe is depressed, but the active is quite regularly depressed; and in the third group, those with severe overloads or those with marked inherited susceptibility, both total and active calciums tend to be low.
Table 13. Average Calcium Levels of Three Typical Health Groups of Eleven, Each on the Basis of Blood Chemistry
A proper discussion of this matter should relate the decalcifying processes, such as we are all familiar with as pyorrhea alveolaris, with their systemic aspects, for we have not adequately realized that these individuals have typical bone characteristics in every part of their body. I do not presume to offer an explanation for the etiology of these metabolism degenerative diseases, but I wish to call your attention to these fundamental basic relationships to the way the individual handles his or her calcium.
It is of particular importance in connection with tuberculosis that those individuals have the losing fight who fail to calcify their tubercles, or who decalcify them if they were calcified; and, conversely, those of us (we are advised by our leading pathologists this includes most human beings) who think we have not had tuberculosis, but who have had and have recovered because we have calcified our tubercles. In connection with cancer and its relation to calcium, I shall later call attention to the fact that, under the stress of depression of the active calcium from infection or otherwise, Nature seems to have a mechanism for dragging that important element up to a higher level by increasing the total calcium.
With this in mind, please note the statement of Dr. Ludwig M. Wolff, sanitary councillor and German cancer specialist, who has recently been quoted in the Science News Letter, September 5, as stating, in a discussion regarding the recent announcements of a germ that will produce cancer, that he is in accord with the thought of the group at Dover, England, which he discusses, saying in part regarding calcium:
“The Dover idea of treatment involves the use of radio-phosphate of potash. This oxidizes the blood and prevents an excess of calcium, that usual phenomenon of middle age, just about the time when cancer begins to rear its head.”
In this connection, it is important to quote from Dr. W. M. Crofton of the Royal Academy of Medicine in Ireland:
“It was suggested that the cancer cell was really of the nature of a phorozoon, the normal cell being degraded to this stage as the result of chronic submaximal stimuli and enabled to live owing to a change in the body fluids. Dr. Crofton suggested that in many cases, if not in all, the stimulus was caused by chronic infection with non-pathogenic bacteria.”
It is exceedingly difficult to visualize this difference in normal and acquired susceptibility without long and intensive study. The boundaries are not sharply defined. However, I have taken the information that has been accumulated in the intensive study of more than 1,600 charts of families, and I have expressed this in Figure 10, in which will be seen the life and illness expectancy of the three susceptibility groups–absent, acquired, and inherited. The portion left plain white expresses the average period of good health, the portion with the lines represents the period of recurring illness and the portion blackened is the part of 100 years which they of that group have not had the privilege of life.
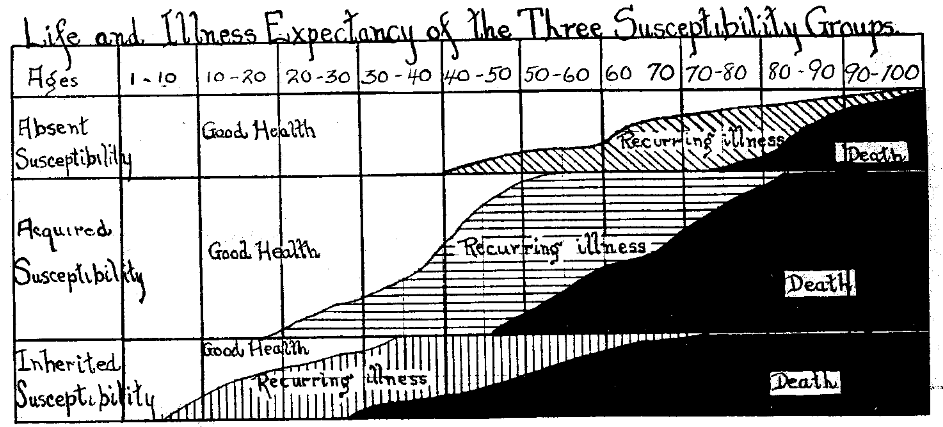
Fig. 10. Comparison of health and disease expectancy in three different groups.
In the inherited susceptibility group, the lines are vertical. They are chiefly disturbed with the so-called rheumatic group affections. This group constitutes approximately 25 per cent of the total population. The period of recurring illness develops in part of the group under 10 years, in a large number between 10 and 20, and in most of them by 40 years of age. Death starts reaping between 20 and 30, and takes its heavy toll before 50, only a few reaching 70.
The middle group with the acquired susceptibility is by far the largest, constituting about 50 per cent of the population of an average community. They under proper care should remain in the group with absent susceptibility, though they do not have so high a defense. Their breaks are caused largely by overloads, of which influenza and pregnancy are the most frequent. They break with certain of the rheumatic group and certain of the nonrheumatic group affections. Their recurring illness period has begun with most individuals by 50 years of age, and death starts its toll at 45, and often occurs under 55 years of age. In this group, we have placed the lines horizontally.
The third group, or those with the absent susceptibility, is made up largely of those individuals, with whom we are all familiar, who boast that they have never had a sick day in their life. While they do not develop the so-called rheumatic group diseases, they do furnish largely the individuals who make the losing fight with tuberculosis, diabetes and cancer, or die finally of old age. Please note I do not state or imply that tuberculous patients have either diabetes or cancer, that anyone of these affections predisposes to another or that all in this group develop one of these diseases. In this absent susceptibility group, we have many individuals living beyond 90 years of age. The average tenure of life for the individuals of this group is approximately twice that in the inherited susceptibility group, but please note there is a marked difference in the span of life in the different individuals in the different groups. The lines are placed obliquely for this group. If, now, we shall presume that, because we can find so many dozens, hundreds or thousands of individuals from the last group who have carried root fillings for 10, 25, or 50 years, we have an illustration of what may be expected to happen in all other individuals, we will make a mistake which is tragic in its injustice, and yet is it not just what the profession has been doing largely in the past?
What I am concerned about is not only the question of the relation of infected teeth to those who are living, but also the question as to the relation of their infected teeth to those who have died. I have not included in this chart the deaths in infancy and from the epidemic diseases of childhood, which would move the age limits much farther to the left. I am in this chart dealing with the individuals who have escaped those handicaps.
I would say, therefore, of the people in these three groups, as illustrated in Figure 10, that those individuals who classify as having an inherited susceptibility should never under any ordinary circumstance have a single root filling, nor should they be allowed to retain one if it is present. They cannot maintain sterility if we could produce it. In spite of everything we can do for them, they will go through life with a tremendous handicap; but just as Eskimos do not die of measles unless they are exposed to measles, just so these may not die from a streptococcal infection if they have not been exposed to strains of the type which will readily produce the lesions to which they are susceptible, and no type of focal infection lesion of the entire body is comparable in danger (because of its mechanical internal and external conditions) to an infected tooth, for the defenses of the body cannot enter the tooth and annihilate the source of toxic and bacterial irritation, nor can Nature absorb the infected dentin sequestrum because of the living cementum about it, which protects it.
The individuals with an acquired susceptibility in the middle group should all, in my judgment, have practically all teeth with root fillings removed by the time they are 45 to 50 years of age, and just as much sooner than that as their overloads shall tend to depress their physical defense. Do not think you can come to their rescue and remove the endangering tooth just before the attack of influenza or other serious overload. The only time to prepare their bark for the sea of life is when it is in your dry dock, not when the ship is in a storm.
Individuals in the upper group or absent susceptibility constitute approximately 25 per cent of all the people of an average community, but since cancer and diabetes and tuberculosis take such a large toll, we must be very careful not to produce in their bodies conditions which tend to increase their susceptibility to these affections. If, however, root fillings or root resections must be made, they should be limited, if possible, to the individuals of this group. It is my belief that even the individuals of this group should have all pulpless teeth removed before they are 55 years of age.
Fourth: The new evidence on the basis of blood chemistry demonstrates the extremely severe injurious effects of dental infections on the defenses of the body.
As unanswerable as the data herewith presented have been, it is significant that an enormous field of new information has been opened through the medium of the study of the changes of the blood of patients and animals under various conditions in relation to dental and focal infections. In the light of these newer data, we are compelled to look on many, if not most, of the degenerative diseases as symptoms and end results of fundamental systemic changes produced in the body by various contributing factors, an important one of which has been focal infection, chiefly from the teeth. It is my belief that these constitute by far the most important argument against temporizing with dental infection. I do not come to you with hearsay or largely quotations, but from a great fund of evidence that has developed directly under my direction, and I therefore speak first hand, and I believe the evidence will speak for itself.
Patients with chronic dental infections have been considered safe or in danger in accordance with the apparent evidence of a serious lesion in heart, kidney, joints or elsewhere, provided it could and had been demonstrated that there was no possibility of focal infection coming from any other part of the body. Then and then only might the dental infections be condemned in the minds of many operators.
That this point of view is not based upon any great truth but is the confidence inspired by ignorance can be abundantly demonstrated. When the crushed infected tooth is washed in physiologic sodium chlorid solution and the relatively clear washings are inoculated into the ear vein of a rabbit, even after the removal of all débris, there is often produced in the animal a progressive series of changes, which find their expression chiefly in blood constituents and their proportions together with a loss in weight and frequently with marked marasmus. It should be noted that there will generally be no localized symptoms as heart, kidney or joint involvement.
That this is not necessarily chiefly due to bacterial content can be demonstrated by a production of even severe expressions with tooth washings that had been put through a Berkfeld filter. Figure 11 shows two rabbits, the upper one of which was inoculated, in its ear vein, with the crushed washings of an infected tooth. It lost 35 per cent in weight in five weeks, while its brother gained 15 per cent in weight.
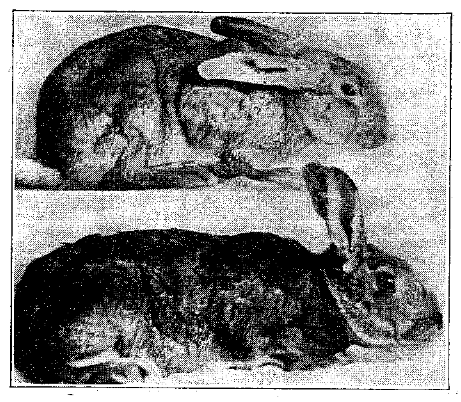
Fig. 11. These rabbits are brothers. The upper, which was inoculated with the washings of a crushed, infected tooth, lost 35 per cent in weight, while the control gained 15 per cent.
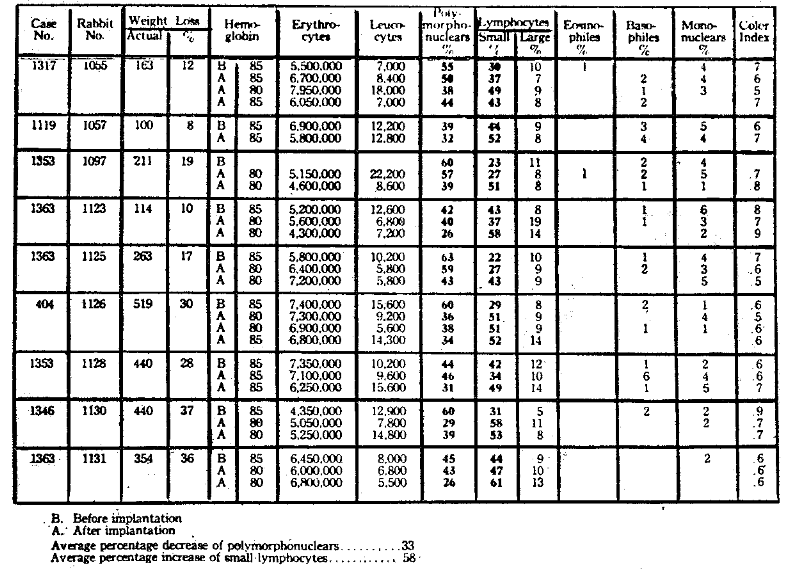
When we study the blood stream changes, we find that quite similar symptoms are produced in animals if the infected tooth, instead of being crushed and its washings injected, is itself passed through a buttonhole incision underneath the skin and the wound closed by proper surgical procedure. Table 14 presents findings in a series of such rabbits, and it will be noted that in each as the animal lost in weight (more in some than a third) there was a progressive depression in the percentage of polymorphonuclears, with a corresponding increase in the number of small lymphocytes. Something was taking place in the animal’s body which was destroying its ability to fight its own infection. This decrease in polymorphonuclears amounted to 17 per cent in the average of the nine rabbits shown in that figure.
Table 14. Typical Blood Picture in Certain Types of Chronic Dental Infection
When we take a single animal and note the change in the readings from day to day, it will be observed (Table 15) that the first effect of the inoculation was an increase of the polymorphonuclears from 57 to 70 per cent, then finally a decrease to 31 per cent in six days, during which time the small lymphocytes increased from 34 to 62 per cent.
Table 15. Comparison of Changes in Ionic Calcium and Blood Morphology Due to Culture Inoculations.*
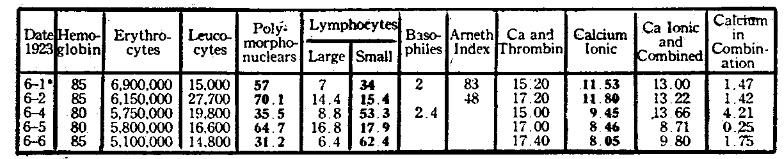
*Before inoculation.
This is in part what happens in very many patients carrying dental infections which they and their dentists think are doing them no harm. Such a group of individuals will be shown in Table 16, in which will be seen a number of patients in whom the polymorphonuclears were depressed much below normal and the small lymphocytes correspondingly increased. There probably is no simple test available in the ordinary pathologic laboratory which will have so great significance and ease of determination in cases of suspected injury to the defenses of the body, without as yet signs of physical break in localized tissues, as has this comparison of the percentage of polymorphonuclears and small lymphocytes.
Table 16. Blood Morphology of Clinical Cases Showing Typical Low Polymorphonuclears and High Lymphocytes
If time permitted, however, I would wish to refer to some other but unusual contributing factors which may contribute to this expression, relating chiefly to disfunction of certain glands of internal secretion.
By referring again to Table 15, it will be noted that the depression of the polymorphonuclears is associated with a change in the active or ionic calcium, which at first increased from 11.5 to 11.8, and then progressively decreased to 8.05. In more than 200 rabbits so tested, approximately 175 have died within a short time. Those that lived did not present this typical picture, nor did they show, as this group did, the development of fluid about the infected tooth. On the contrary, those that lived invariably built a fibrous, highly vascularized capsule about the tooth, which adequately encapsulated it and which became in effect a quarantine station.
The activity of the leukocytes of the body, which are not only the chief phagocyting cells, but, which is much more important, furnish the bactericidins for the defense of the body, has been demonstrated by Hamburger and others to be chiefly dependent on the level of the calcium. In animals with a low calcium, it can be easily demonstrated that there is a depression of this factor by the simple procedure of placing the open end of a minute capillary tube of infected culture medium beneath the skin. The leukocytes will progress into the lumen approximately a half inch in two hours, if the rabbit has a normal calcium level, but will not travel more than half that distance if there is an active calcium level that is depressed from 10 to 20 per cent below its normal.
If calcium lactate is introduced into the rectum of such a rabbit, it will, in less than an hour, show an increase in the rate of migration of the leukocytes, as they are induced by chemotaxis to progress into the tube to the organisms.
Dr. Price (in rebuttal): No one will have surmised, until he has been informed, the tremendous significance and importance of calcium in the various physiologic processes of the body, in plant life as well as in animal life. Even the rate of heart beat and the strength or volume is largely influenced and controlled by the level of the calcium in the blood and tissues. Every organ of the body has a depression of its function with a depression of the blood calcium and may be hyperactive when the calcium level is too high. Irritability of the nervous system is largely the result of imbalance of the body’s mineral constituents. The neuralgias and forms of neuritis are in large part expressions of disturbed calcium level.
It is not so simple a matter, however, as is generally thought, as merely a measure of total calcium; on the contrary, the total calcium may be amply high and the animal or individual be perishing for want of available calcium.
Time does not permit an adequate review of even the major fundamentals as at present known. We at present determine five distinct calcium factors besides three relating calcium, inorganic and organic phosphorus. Of the total calcium of the blood stream, a part is in colloidal form as a proteinate (a globulin compound). This collodial calcium is nondiffusible: that is, it does not diffuse through certain tissues because the molecule is too large. Another fraction of the total calcium is diffusible and is available for tissue uses and chemical combinations. A certain factor including most of the diffusible, and generally some additional, is spoken of as active or ionic because it can readily take part in certain biologic reactions such as inducing the clotting of blood.
The inorganic phosphorus is, like the calcium, of fundamental importance. The product of the inorganic phosphorus and total calcium and the product of inorganic phosphorus and the active calcium furnish factors which directly express the level of the calcium balance and therefore a measure of the vital capacity.
An infected pulpless tooth in an individual causes, in greater or less measure, that which we have shown to occur in rabbits when an infected tooth is placed beneath the skin. This condition may exist for months or even years, constituting a menace to the calcium balance of the body and thereby undermining the defense or immunity without the patient or his dentist physician having the slightest indication or even suspicion of the condition, on the basis of the former and largely current methods of interpretation; for such teeth in such individuals are not sore and may have little or no roentgenographic involvement.
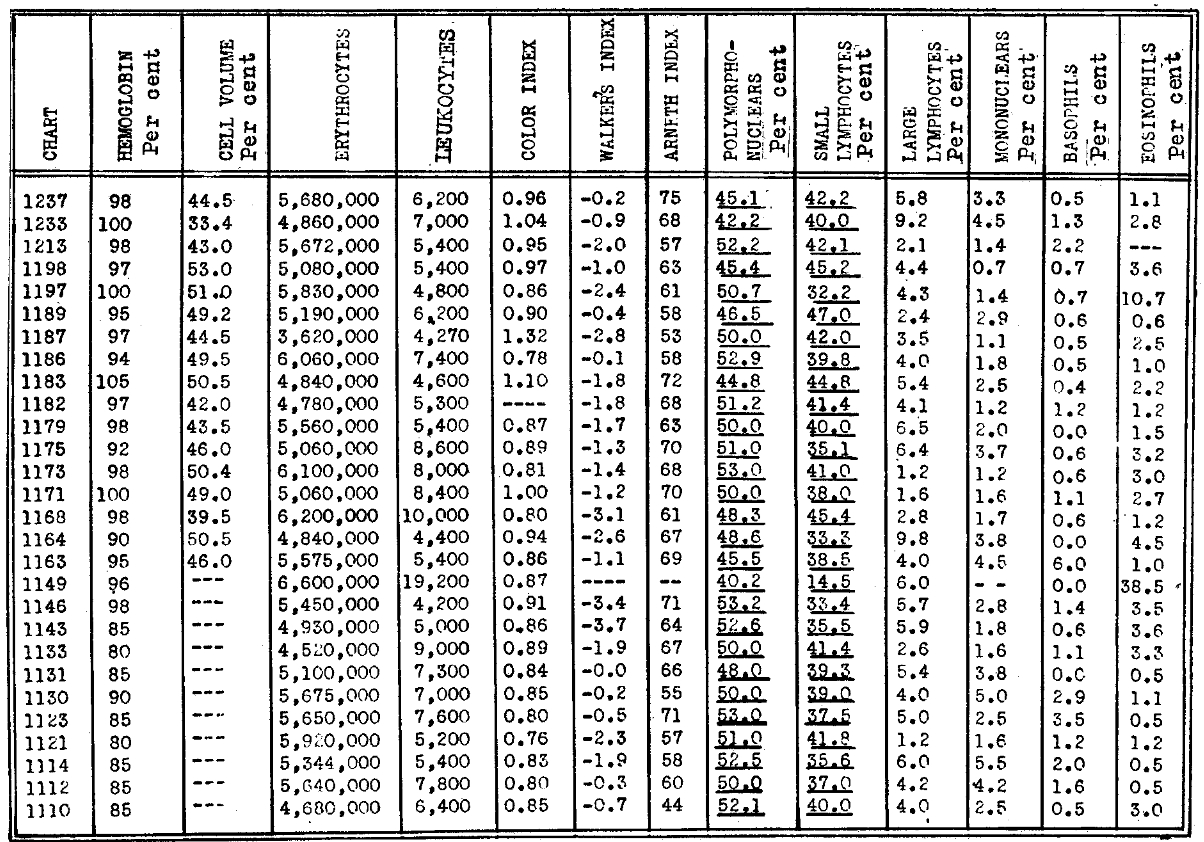
We can learn much from the study of animals and thereby help in the interpretation of what we find in human beings. In Figure 12, an ordinary infected tooth was placed beneath the skin of a rabbit, and certain changes developed in the blood stream, particularly in the calcium and phosphorus. The total calcium progressively decreased during the first nine days, during which time the active calcium underwent a very great reduction, falling about one half. Our previous experiments with large numbers of such animals have demonstrated that they die in convulsions when the active calcium is reduced to about 5 mg. An abscess had developed about the implanted tooth about as big as a hen’s egg. The two lines showing total and active calcium balance both became depressed below the zero line.
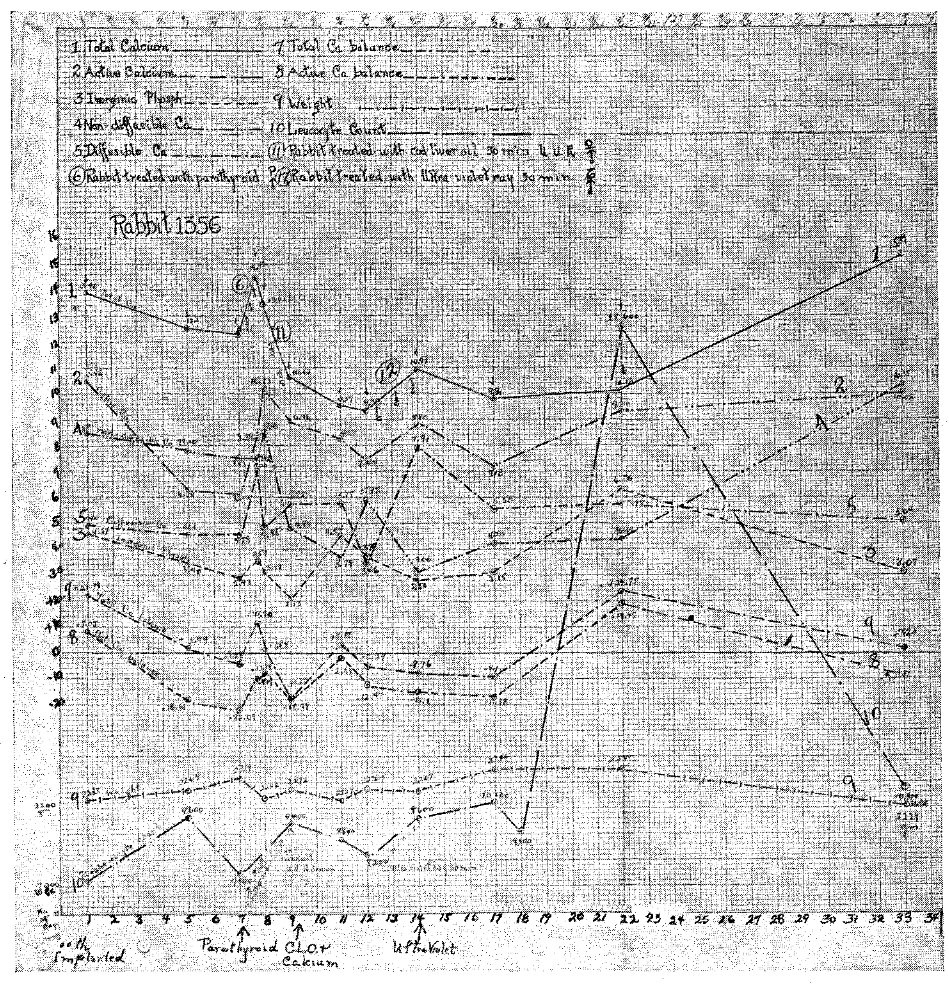
Fig. 12. Changes produced in various blood factors by placing infected tooth beneath the skin of the rabbit: 1. Total calcium. 2. Active calcium. 3. Non-diffusible calcium. 4. Diffusible calcium. 5. Inorganic phosphorus. 6. Total calcium balance. 7. Active calcium balance. 8. Weight. 9. Leukocytes (Rabbit 1356). Note marked changes, especially of active calcium and response to treatments.
The animal was given treatments, which time does not here permit the detailed explanation of, for the raising of its calcium. This resulted in a change of the levels of calcium balance from below the zero line back to approximately normal, the swelling spontaneously decreased and the tooth became encapsulated. The animal was temporarily rescued, as are many people. As time progressed, however, it lost in weight and its calcium balance was slowly lowered. Unless its body is reinforced again by medication, it will succumb to the slowly overwhelming toxic infection which it has not the capacity to neutralize unless assisted from some outside source. Nature, in her heroic effort to hold up the depressing calcium factors, proceeds to raise the total calcium. As in many people with infected teeth, the mechanism of defense in this animal is slowly but surely breaking, and it, like them, will become an easy prey to infection. The balance will always be determined in part by the contributing overloads. This animal, from the direction of the negative calcium balance and body graphs, is doomed.
When we compare the record of this rabbit with the record of another (Fig. 13), which was similarly treated at the same time, we find, in general, the same progress except that, in the latter, the animal was not so rapidly overwhelmed, and, in order to hold up the depressing various calcium factors, the total blood calcium was increased under treatment. The animal rallied, only to start declining again.
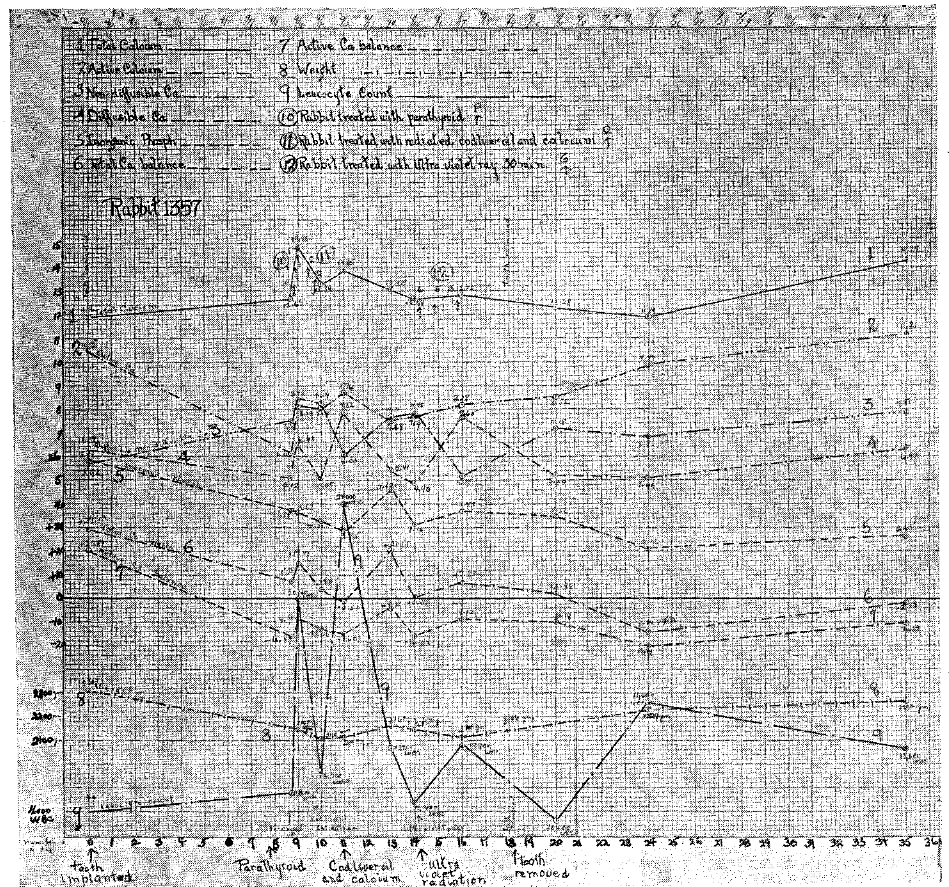
Fig. 13. Rabbit 1357. Similar treatment to that shown in Figure 12 was given. The tooth was less toxic. Note rise in total calcium with fall of active calcium and rapid improvement with removal of tooth.
At this time, the infected tooth was removed from beneath the rabbit’s skin, and it proceeded thereupon to show a change in all the blood factors. The negative calcium balance and body weight, and in fact all the various factors, steadily progressed back toward normal.
Those who do not understand the closeness with which pathologic pictures will be produced in human beings and in animals with like causes will not expect that we will so often see in our patients just such changes in blood stream chemical factors as have been produced in these experimental animals.
Time and space will only permit of one illustration, of which we have many. A patient suffering from neuritic pain in the right shoulder and digestive disturbance, which had been getting progressively more severe for two years, was at the time he came in virtually incapacitated. (Fig. 14.)
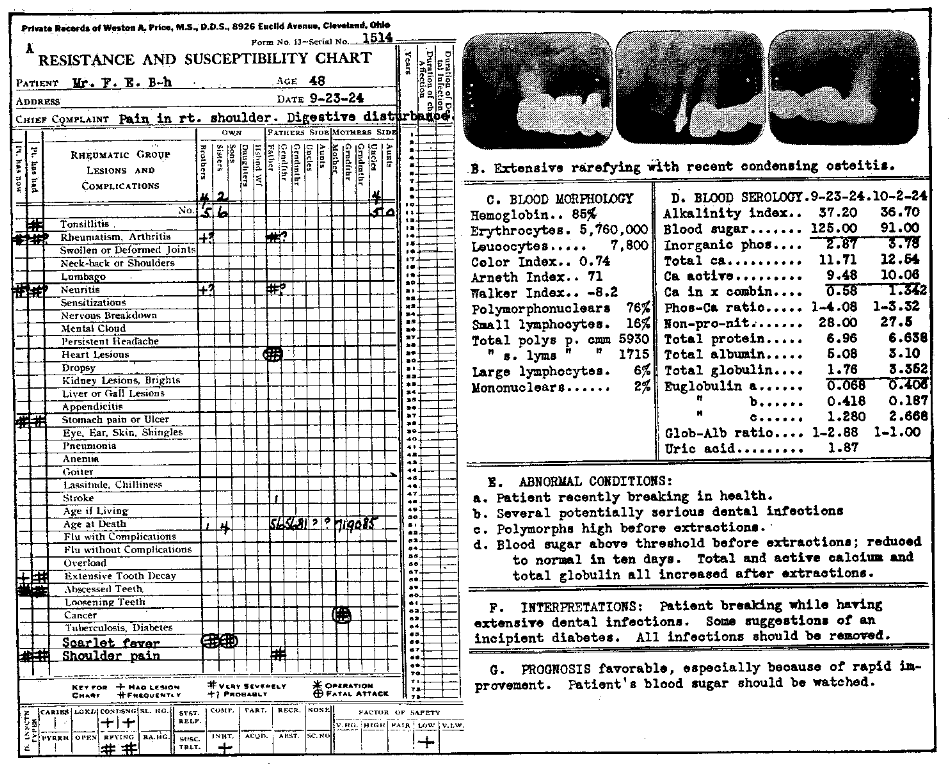
Fig. 14. Typical blood-chemical change produced in a patient by removal of dental infection.
With the removal of chronic dental infection, there was, in ten days, the remarkable change shown in the chart. The total calcium increased from 11.7 to 12.5; the active calcium from 9.4 to 10; the inorganic phosphorus from 2.6 to 3.7; and the total globulin from 1.7 to 3.3. The blood sugar was reduced from 125 to 91.
With these changes, there has been a complete return to normal health. We have recently seen him and he reports that he returned promptly to business after the removal of the dental infection and for approximately a year has continued in good health.
The total calcium balance of this patient changed from a negative calcium balance of -7.3 to a positive calcium balance of +6.2, and the active calcium balance changed from a negative of 13.6 to a negative of 3. The globulin-albumin ratio changed from 1:2 before, to 1:1 after, which is approximately normal.
This remarkable improvement occurred in ten days after the removal of his chronic dental infections. It is of particular importance to note that this patient was suffering from digestive disturbance of increasing severity prior to the removal of the dental infection, and that this disturbance entirely disappeared with the removal of dental infection and he was able to return to a full, mixed general diet.
Similarly, a patient, 61 years of age, suffering from marked lassitude and physical and mental depression, experienced the following changes in his physical condition twenty-seven days after the removal of dental infection: The alkalinity index was raised from 33.4 to 36.7; the organic phosphorus, from 3.5 to 4.1. The nonprotein nitrogen, which was very high at 40, decreased to 30; the total calcium increased from 9.7 to 11. The active calcium, which was very low at 8.5, increased to 9.4. The total calcium balance, which was -4, increased to +5. The active calcium balance, which was 9, decreased to less than 1. With these blood changes, the patient’s health so greatly improved that he considered himself well back to normal.
I hope I am making it clear, both that the disturbances of the normal levels of the chemicals of the blood are a part of the general condition, which we have been used to seeing chiefly or only as clinical symptoms, and also that, when these conditions exist for an extended period, they tend definitely to contribute to the degenerative diseases, though they may exist as disturbances and measurable changes in the blood stream for months or years before the clinical symptoms become manifest. When they do become manifest, they often constitute degenerative diseases so far advanced that even the removal of dental infection cannot correct them. The injury to heart and kidney tissue, for example, has been so serious that complete repair and complete recovery may be impossible, though it might have been prevented in part or in whole by removal of the dental infection before the secondary expression has seriously manifested itself in the essential organ. We are coming more and more to look on the degenerative diseases as symptoms of these various contributing factors.
This is the treatment indicated for our patients with infected teeth, if we would conserve what is more precious to them than even their natural pearls: those factors which determine the efficiency of their defense against overload and infection. This, in other words, is the time and the way an enlightened dental profession, enlightened by a new sense because it has a new truth, will treat heart disease, kidney disfunction, and general degenerative processes.
Dr. Price (closing): If, now, we summarize these various presented data, we find that:
- People are not living nearly to the entire span of life which they have a right to expect:
- Death is occurring even in our most civilized communities largely from the degenerative diseases, chief of which is heart disease.
- Even the mortality statistics of our various communities will at this time give an indication of the level and thought of dental practice with regard to the management of infected pulpless teeth.
- It is practically, if not entirely, a physical impossibility to sterilize infected cementum by treating through the dentin. It is like trying to sterilize infection in the label on the bottle by putting disinfectants in the bottle.
- Root fillings do not continue to fill root canals. The amount of space that ultimately develops is approximately the amount of solvent that was used with the root-filling material, assuming that mechanical filling of every area was possible.
- Individuals are not comparable in their defense against degenerative diseases. Some are susceptible and must have an entirely different preventive program.
- The degenerative diseases are largely symptoms of degenerative processes in the blood stream, an important contributing cause for which is long-continued, usually unsuspected, chronic infection.
The extremely inadequate time and space for this statement prevents the inclusion of similar important evidence, demonstrating that:
- The roentgen rays cannot reveal all the required information, and under old standards will often be misleading.
- The complement fixation method for dental infections can be related to systemic sensitization.
- Chronic dental infections reduce the normal bactericidins of the blood.
- Leukocytic activity is depressed by chronic dental infections.
- Chronic dental infections can produce antigens, to which the sensitized patient may respond with an allergy of severe and very obscure type.
- Dental infections can be demonstrated to have had specific localizing ability for many of the organs and tissues of the body. I have already reported on most of these in my papers and books.
We cannot, therefore, continue in the light of these new truths to give any quarter to the infected pulpless tooth until we can both accomplish its disinfection and insure its continued sterility. Until then, it must be eliminated. By the elimination of dental focal infections, we will eliminate one of the important contributing factors to the shortening of life and loss of health, for it is chiefly the destructive influences of these infection products that have to do with the destroying of the defensive mechanisms of the blood stream and the producing of abnormal levels, chiefly of calcium, which thereby predispose to sensitization reactions, cancer, tuberculosis, diabetes and the anemias, on the one hand, and to the rheumatic group of degenerative diseases on the other, two groups which together constitute the great majority of deaths in the various communities.
A new truth is a new sense, for, with it, we can see things that we could not see before and things that cannot be seen by those who do not have that new truth; but a new truth comes only to a prepared mind, and for those of us who have in some degree a prepared mind, we are able to say with Ross, for we can see with this new truth the thing that he could see when he found a means for relieving malaria:
This day relenting God
Hath placed within my hand
A wondrous thing; and God
Be praised…
I know this little thing
A myriad men will save.
In closing, I want you to see with me a little incident that happened in a town in Illinois, a year ago last Christmas. Prior to that time, there had been appearing, in a window, a little hand that seemed to wave to each passing train as if in distress. At night, a flickering match took its place, and it was waved frantically as a signal for help.
This got on the nerves and hearts of the trainmen as they passed by; and as they exchanged reports, they decided that there must be someone there in distress. Accordingly, a committee was appointed to go and investigate; and it was found that a little bedridden child lay crippled where she could not see out of the window but where she could reach her hand in front of the window.
On Christmas morning, two transcontinental express trains stopped on the main line in front of this little home, and from them committees of trainmen proceeded to the little home to carry comforts and money to help this afflicted little sister of humanity.
I do not know what she was suffering from, but I do believe that there are many such sufferers who have been an important, if not a controlling, contributing factor in dental infections, and I am going to ask that every time you place a root-filling in an infected pulpless tooth, you shall see that hand waving in the window.
References Cited:
- Brooks, Matilda M., and Price, W. A.: “Relative Efficiency of Medicaments for the Sterilization of Tooth Structures,” J.N.D.A., 5: 273 (March) 1918. Price, W. A.: Dental Infections, Oral and Systemic (Vol. 1) Chap. 14.
- Price, W. A.: Dental Infection Oral and Systemic.
- Price, W. A.: Dental Infections, Oral and Systemic, Chap. 2.