
Access to all articles, new health classes, discounts in our store, and more!
Why the Human Face Is Shrinking

Today, we are faced with an epidemic of micronutrient deficiencies, resulting in deficient human growth patterns. These growth patterns often first manifest clinically as a small palate or upper jaw, a condition correctly termed maxillary dysmorphogenesis. This condition actually affects the functionality of the mandible (lower jaw) and the whole head and neck. Small palates have serious jaw, ear, cranial, airway, and postural consequences, and, as a result, about 60% of children today will need palatal growth assistance or expansion orthodontics. As my teacher and orthodontic confrere, Dr. Lawrence Funt, used to say, “The maxilla is the criminal, the mandible is the victim.”
This change in human growth patterns is caused by current, widespread dietary micronutrient deficiencies that make up what I call dietary deficiency dysfunctionality dysmorphogenesis syndrome. These deficiencies are due to such factors as a deficient maternal nutrient supply – caused, in part, by poor maternal macronutrient food choices, massive worldwide soil nutrient depletion, and the recent introduction of a large number of metabolic disruptors in nutrient-deficient processed foods – combined with a dangerous decline in breastfeeding. All of these factors lead to imperfect epigenetic expression of the human genome. In other words, we do not get ideal developmental expression. This article explains why the human face is shrinking and why this results in numerous health problems.
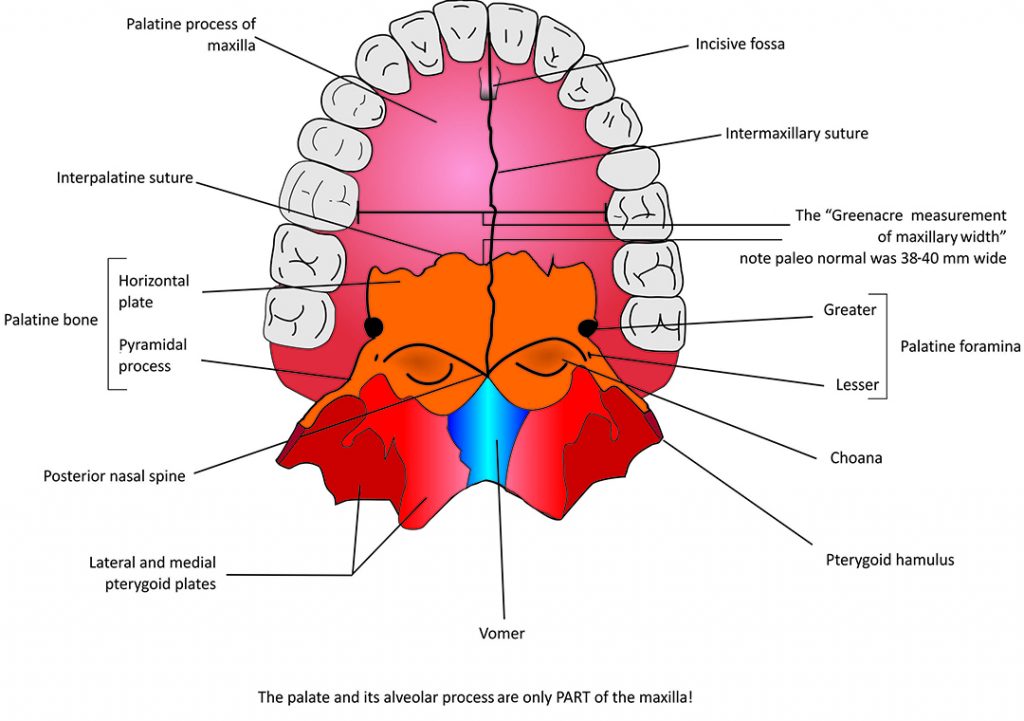
One of the first obvious indicator areas of skeletal dysmorphogenesis is the shape or width of the palatal arch, the bony arch at the roof of the mouth. Maxillary dysmorphogenesis starts when the maxilla starts forming at about 8½ weeks in utero. No one presently that I know of, in clinical medicine, is measuring the width of the palatal arch in medical diagnosis. This is a major medical oversight, as this measurement provides vital diagnostic information. It is a key cranial bone marker that is being overlooked by all health practitioners worldwide. I am, in this article, formally declaring maxillary dysmorphogenesis as the newest medical dysmorphogenetic diagnostic clue, or the “canary in the cranium.”
The first consequence of a small upper jaw is that it disturbs lower jaw posture, and creates dysfunction of the two jaw joints as a direct result. If the lower jaw grows properly to be full sized, how can it fit into an undersized maxilla? Problems develop if you try to put a size 9 mandible into a size 6 maxilla. This is why everyone knows about temporomandibular joint (TMJ) problems. ENT specialist Dr. Henry Uhlemeyer said, “In my opinion, the mandible is the electrical control coordinator of the body.” He went on to observe that “if the mandible is not physiologically positioned, all stress hormones are automatically stimulated…blood pressure rises, blood sugar rises, [and] the GI tract responds acutely.”[1]
A 1993 study looked at maxillary dysmorphogenesis in relation to TMJ dysfunction, retrognathia (a condition in which the lower jaw is set back further than the upper jaw), and midline distortions. This groundbreaking retrospective MRI study of 128 children 14 years of age or younger was designed to “evaluate the relationship between internal derangements of the temporomandibular joint(s) (TMJ) and disturbed facial skeleton growth (dysmorphogenesis).”[2] The researchers, two radiologists, concluded that TMJ derangements are common in children and may contribute to the development of retrognathia (causing bad bites or orthodontic problems).
When an underdeveloped palate causes a posteriorly displaced lower jaw, forward head posture can result, so that the cervical vertebrae are stressed and displaced. Dr. Steven Olmos published a clinical study in 2005 that confirms jaw posture influences forward head posture.[3] Consequently, bad jaw posture most likely means that the whole spine suffers. Quite simply, a smaller upper jaw and a subsequent bad bite will influence spinal growth and alignment, leading to abnormal spinal curvature, such as lordosis, scoliosis, or kyphosis. In other words, I think that the head will not balance well and the spine will not function well if the palate is underdeveloped and the mandible becomes dysfunctional.
 Micronutrient deficiencies also mean that the female pelvis will probably not develop as widely as intended, without full pelvic brim development to facilitate traditional vaginal deliveries. This may lead to a greater need for C-sections. One astute Australian obstetrician, Dr. Kathleen Vaughn, told Dr. Weston A. Price that she could usually predict which women would need a C-section by looking at their faces, their crowded teeth and smaller jaws, and the nature of their gait due to their narrow, underdeveloped hips.
Micronutrient deficiencies also mean that the female pelvis will probably not develop as widely as intended, without full pelvic brim development to facilitate traditional vaginal deliveries. This may lead to a greater need for C-sections. One astute Australian obstetrician, Dr. Kathleen Vaughn, told Dr. Weston A. Price that she could usually predict which women would need a C-section by looking at their faces, their crowded teeth and smaller jaws, and the nature of their gait due to their narrow, underdeveloped hips.
We must also consider the extensive obstructive sleep apnea (OSA) evidence accumulated by the amazing renaissance sleep researcher Dr. Christian Guilleminault and his colleagues at Stanford University, who concluded that “pediatric OSA in non-obese children is a disorder of oral-facial growth.”[4] A more recent article also supports the dysmorphogenesis theory, stating: “Investigation of fetal development and early-in-life orofacial growth allows recognition of risk factors that lead to change in upper airway patency, which leads to abnormal upper airway resistance, abnormal inspiratory efforts, and further increase in resistance and progressive narrowing of the collapsible upper airway.… Recognition of the problems should lead to appropriate treatments and prevention of obstructive sleep apnea and its comorbidities.”[5]
Furthermore, the work of world-renowned orthodontist Dr. Derek Mahony suggests links between maxillary dysmorphogenesis, airway insufficiency, sleep-disordered breathing, and symptoms resembling ADHD. He has seen many children with oral myofunctional disorders and sleep-disordered breathing who were able to be taken off their ADHD medication after being successfully treated with orthodontics.[6]
Dr. William Hang, a California orthodontist, has said, “When the orthodontic profession quits focusing on straight teeth and focuses on optimizing both forward facial growth and airway, it will finally become part of health care.”[7]
Maxillary dysmorphogenesis may also be related to brain dysmorphogenesis and dysfunction, including schizophrenia. In one study, Delice et al. stated, “As the palate develops in conjunction with both the face and brain, our study findings can significantly contribute to the assumption that there might be structural abnormalities of the palate that could represent specific markers of embryological dysmorphogenesis underlying schizophrenia.”[8]
Other researchers, such as Waddington et al., have also seen a correlation: “In the context of human developmental conditions, we review the conceptualisation of schizophrenia as a neurodevelopmental disorder [and] the status of craniofacial dysmorphology as a clinically accessible index of brain dysmorphogenesis.”[9] In addition, Buckley et al. noted, “Subtle dysmorphogenesis of the craniofacial region constitutes important corroborating evidence of the neurodevelopmental origins of schizophrenia.”[10] However, these findings are not well known in dental or medical clinical contexts.
I believe that maxillary dysmorphogenesis is an anthropological and growth-deficiency tragedy, although both doctors and dentists usually overlook the problem. Further, my contention is that musculoskeletal dysmorphogenesis first shows up clinically in smaller maxillae. Thus, dentists and doctors need to look more closely at human structural changes and start doing palatal measurements on all their patients. This will greatly facilitate diagnosis of maxillary dysmorphogenesis and its powerful total body consequences.
All doctors should measure the width of each patient’s palate from the lingual of the upper right first-year molar to the lingual margin of the upper left first- or six-year molar as a clinical marker in their diagnostic protocol. Very good maxillary width is 38 to 40 mm. Very poor maxillary width is 28 to 36 mm. The latter is the range usually seen clinically.
In addition, doctors can measure the vertical range of motion of the patient’s jaw joints by asking them to put three fingers together and place them vertically between their upper and lower teeth. If they can do this, their jaw joints are functioning normally. If they can only open to two finger widths, the joint function is dysfunctional. It might also be useful to observe if the mandibular midline is congruent with the maxillary midline. (Doctors can email me at [email protected] for clinical training.)
Causes of dysmorphogenesis
Why do humans not naturally grow wide, healthy palates today, as they did two million years ago? Dr. Clark Spencer Larsen, professor of anthropology at Ohio State University, observed, “Over the past 10,000 years there has been a trend toward rounder skulls with smaller faces and jaws.”[11] Anthropologists know that human palates, faces, and pelvises are shrinking, but they do not know why. Although humans now have noticeably narrower skulls and airways, the skulls and jaws of other mammals, such as dolphins and gorillas, have not changed. What are we doing wrong? Perhaps this is all part of a larger, overlooked problem – dietary deficiency syndrome.
Historically, humans and our hominid ancestors consistently grew great, wide jaws with an almost edge-to-edge bite for about two million years. These jaws grew to be very functional and very healthy. The simple, mainly raw diet and consistent tongue-to-palate swallow pattern essentially empowered all this magnificent palatal and facial growth. However, our civilized diet and modern cooking and child-feeding practices have changed this pattern of growth for the worse.
I believe that micronutrient deficiencies, changes in infant feeding, poor food choices by families, and the introduction of myriad metabolic disruptors over the last hundred years are the causes of numerous chronic and acute dysmorphogenetic human maladies. Maxillary dysmorphogenesis is simply the first and most obvious clinical marker.
Here are the top ten probable reasons for maxillary dysmorphogenesis and the increasing incidence of dysmorphogenesis in general:
1. Pathologic changes in how modern humans swallow
Our habit of using artificial nipples in the feeding of infants has created a lot of pathologic or poorly directed swallows. The hypoglossal muscle becomes mistrained when we use badly designed and unphysiologic round latex nipples in bottle feeding. This means the tongue does not consistently push up and forward on the developing palate to stimulate proper palatal growth, and the palate and its two separate lateral growth plates do not grow to their full genetic potential. Breastfeeding and a powerful swallow are the architects of a good palate, and this all leads to a healthy life.
2. Micronutrient deficiencies in our food supply due to soil depletion
Instead of traditional, organic farming methods with all the trace minerals being replaced in the soil, we now mostly farm chemically with poor fertilizers and dangerous herbicides. This is contributing to soil depletion, leading to weak plant life and subsequently fewer trace minerals, vitamins, amino acids, enzymes, and essential fatty acids in our bodies. As Dr. Charles Northern, an Alabama MD who dedicated his life to studying soil depletion, said, “Sick soils mean sick plants, sick animals, and sick people. Physical, mental, and moral fitness depends largely upon an ample supply and a proper proportion of the minerals in our foods.”[12]
Sadly, many children are deficient in trace minerals and other nutrients today. Doctors could measure mineral deficiencies easily by sending out baby teeth or hair samples for mineral assay. Teeth are the most mineral-dense structures in our bodies, and both baby teeth and adult teeth could provide us with an exact record of any trace minerals that we lacked during prenatal and post-natal development.
There is some good clinical evidence that hair analysis can reliably identify trace mineral deficiencies, according to obstetrician-gynecologist Dr. Robert Thompson.[13] His number one clinical diagnostic test is HTMA, or Hair Tissue Mineral Analysis. Dr. Thompson believes strongly in consuming unrefined salts or ionic trace mineral supplements daily to correct such mineral deficiencies, in addition to eating as well and as naturally as possible.
Modern functional medicine clinicians and researchers believe that they can better understand our present diseases and predict future disease tendencies by knowing our trace mineral deficiencies. We should be using information about minerals more in medical and dental diagnostics.
3. Reduced breastfeeding
According to the American Academy of Family Physicians (AAFP), “Breast milk offers medical and psychological benefits not available from human milk substitutes. The AAFP recommends that all babies, with rare exceptions, be breastfed and/or receive expressed human milk exclusively for the first six months of life. Breastfeeding should continue with the addition of complementary foods throughout the second half of the first year. Breastfeeding beyond the first year offers considerable benefits to both mother and child, and should continue as long as mutually desired.”[14]
The Academy of Breastfeeding Medicine states, “A vast body of research has demonstrated significant nutritional, physiological, and psychological benefits for both mothers and children that last well beyond infancy. But while breastfeeding is the foundation of a lifetime of health and well-being, clinical practice lags behind scientific evidence.”[15]
I believe that all children should start life as breastfed babies and then progress to bone marrow and bone broths. We stress our infants’ microbiomes by introducing solid foods too early. The human is the only mammal that does not breastfeed and gives their infants milk of a remote species. Breastfeeding should be every human’s birthright. This is health measure number one for a child.
4. Poor macronutrient food choices
We consume far too many sweet drinks, refined sugars, synthetic sweeteners, and nonfoods from the junk food industry, along with too much chlorinated tap water. These substances are dangerous to human health and our microbiome. We should consume more enzymes, essential fatty acids, trace minerals (including iodine), green foods such as moringa, pink Himalayan sea salt, and alkaline ionized water. (Email me for a copy of my nutrition book, E – F.O.O.D.S., ME – F.O.O.D.S., SEA-F.O.O.D.S. and Paleo-Moderns.)
Contrast modern fast food with the diet of Stone Age man. Early humans used stone clubs to smash open bones left behind by animals to get to the bone marrow within, and they ate mostly enzyme-rich raw foods. Traditionally, many native American tribes would transition a breastfeeding infant onto bone marrow from deer or moose. Most modern cooks do not use soup bones as much as our grandparents once did. It would behoove us to drop in regularly at our local butcher shop to buy some canoe-cut bones for a bone marrow “treat” and make bone broth soup. Many New York restaurants now feature a bone marrow canoe cut entrée, and Chef Victoria Blamey has created a bone marrow burger.
5. Metabolic disruptors in our diet and environment
We have added over 100,000 new chemicals to our food, soils, water, and air since World War II. Many of these are metabolic disruptors, which disturb human growth and development. One of the most damaging is the herbicide glyphosate, a known endocrine disruptor whose massive use is correlated with increased risk of numerous diseases.[16] Dr. Norm Shealy expresses his very serious concerns about glyphosate usage in his newsletter, available at normshealy.com.
Excitotoxins such as monosodium glutamate, aspartame, cysteine, hydrolyzed protein, and aspartic acid are also metabolic disruptors and can be toxic to our neurons. The best book written on this subject is Excitotoxins by neurologist Dr. Russell Blaylock. In one journal article, he explained: “There is a strong connection between dietary and endogenous excitotoxin excess and neurological dysfunction and disease.”[17]
Dr. Blaylock also elaborated on in utero issues: “Of particular concern [are] the toxic effects of these excitotoxic compounds on the developing brain. It is well recognized that the immature brain is four times more sensitive to the toxic effects of the excitatory amino acids as is the mature brain. This means that excitotoxic injury is of special concern from the fetal stage to adolescence.”
Sugar is simply a metabolic poison of the first order. Dr. Robert Lustig, professor of pediatric endocrinology at the University of California, called for sugar to be treated as a toxin, like alcohol and tobacco.[18] We consume far too much sugar, increasing our risk of diabetes and other diseases. In the future, all bags of sugar should be labeled “toxic to humans”!
6. Increased allergies and food sensitivities
Allergies can change the pattern of children’s facial growth by causing stuffy noses and mouth breathing. Consider all the kids with open mouths and long faces. They are mostly victims of environmental allergens, sugar poisoning, or metabolic contamination. Blocked noses are signs of lymphoid reactions to the wrong foods. Today, there are many childhood allergens and perhaps even in utero metabolic or nutrient stresses predisposing children to allergies. In addition, many physicians suggest that we introduce questionable solids that are potential food allergens too early to our infants.
7. Insufficient use and stimulation of the jaws
It also may be that we are experiencing disuse atrophy because we don’t chew enough to stimulate full growth anymore. It is true that we do not chew as heavily or as heartily as we used to. Paleolithic humans chewed bones to obtain the marrow, and animal hides to make them more flexible for use as clothing. Jaw muscles simply are not used as much as they were in the time of our hunter-gatherer ancestors. This might contribute to smaller jaws and faces.
Both palates and noses are getting measurably narrower, and this causes maxillomandibular dysfunction as well as nasal and hyoid bone problems. Lower jaw displacement can contribute to airway distress and myoneurologic and myofascial difficulties and can even contribute to the incidence of epileptic seizures. Dr. Dwight Jennings of Alameda, California, is a world expert on the connection between jaw misalignment and release of the neuropeptide known as substance P from the trigeminal nerves. He has shown how a bad bite can influence epilepsy and movement disorders. Substance P may also be a factor in metabolic health and cancer development. (From personal communications with Dr. Jennings in February 2020.)
8. Soft tissue restrictions and oral habits
Frenum ties, both lingual (tongue tie) and labial (lip tie), are often undiagnosed or untreated. These soft tissue restrictions mean that the tongue cannot empower palatal growth. These restrictions can have a significant effect on the baby’s ability to latch on and breastfeed. Midwives a hundred years ago treated these problems within minutes of a child being born.
Researchers Takayuki Kuroda and Takashi Ono stated, “Oral dysfunction, including thumb sucking, mouth breathing, and infantile swallowing, leads to abnormal growth and development of craniofacial structures…. Oral dysfunction may cause changes in the craniofacial skeleton and may affect craniofacial muscular function.”[19]
As Nobel laureate Albert Szent-Györgyi said, “If structure does not tell us anything about function, it means that we have not looked at it correctly.”
9. Microbiome dysbiosis
Newborns are not developing the proper gut bacteria to produce the enzymes needed to properly digest foods. Our micronutrient status is not determined solely by what we eat. It also depends on what we can liquefy and absorb via enzymatic and microbial action in the digestive tract. The development of the neonatal gut microbiome is influenced by multiple factors, such as delivery mode, feeding, medication use, hospital environment, maternal gum disease, drinking water quality, early life stress, and genetics.[20]
10. Birth traumas
Birth traumas and subsequent craniofacial bone displacements may now be major factors in the development of malocclusions. According to osteopath Maryse Tassé of Ottawa, Canada, every newborn would benefit by being seen by an osteopath shortly after birth.
One world expert on craniofacial distortion is the Canadian orthodontist Dr. Gavin James, who recently had this to say:
“As an orthodontist, in a long search for answers, I have come to realise that steps towards preventing or correcting a malocclusion can be taken long before I would normally see a patient. There are three anomalies in particular which may cause malocclusion but which are not seen as an orthodontic responsibility. The first one is craniofacial displacement and trauma sustained by the infant during birth. The second is limitation of function due to soft tissue restrictions, particularly of the tongue. The third is partial or complete obstruction of the nasal and/or pharyngeal airway.
“This is not to ignore the relevance of heredity as a contributory factor or the effects of dietary change as seen in the work of Weston Price.”[21]
Dr. Price was right
We should now look at the importance of the maxilla and its development through the eyes of a great researcher, Weston A. Price, DDS, who went on a worldwide odyssey to study human palates and jaws and the effect of diet on jaw growth. Every physician, dentist, and healthcare worker should read his book Nutrition and Physical Degeneration. In summarizing his study of the beautiful, wide palates of traditional cultures that were not exposed to the modern diet, Dr. Price said:
“Probably the most indelible impression that is left by my investigations…is that which came from examining 1,276 skulls of the people who had been buried hundreds of years ago along the Pacific Coast of Peru and in the high Andean Plateau without finding a single skull with the typical marked narrowing of the face and dental arches that afflicts a considerable proportion not only of the residents in modernized districts in Peru, but in most of the United States and many communities of Europe today. I know of no problem so important to our modern civilization as the finding of the reason for this, and the elimination of the cause of error.”[22]
This last sentence sums up his life’s work, of which every family should be aware. Dr. Price was right, and he is still right. The human face is shrinking. Jaws and faces are getting narrower. We should all know why this is occurring and understand how to reverse this pathological trend. I believe that the key to correcting it is to keep our natural tongue-to-palate swallow, breastfeed our children, use no artificial nipples, and consume more enzymes, trace minerals, alkaline ionized water, and good fats in our diet. We should make liberal use of great foods such as moringa, seaweed, bone marrow, and bone broth soups.
Today, few if any medical practitioners or researchers are considering the importance of the growth and development of the palate. Our palates form the anatomical basis for our airways, sinuses, eye sockets, and noses, and they determine our facial form and the structure of our cheekbones. Maxillary dysmorphogenesis due to dietary deficiency syndrome leads to a long list of major health problems for the growing child, who will continue to suffer for a lifetime if the palate and jaws are not corrected osteopathically and orthodontically.
Dentists and orthodontists see fewer and fewer well-developed maxillae these days. However, they do not see this for what it really represents – a major nutritional deficiency epidemic. When we recognize it as such, we can feed our children differently to reverse this scourge of shrunken palates and faces, dysfunctioning brains, and underdeveloped pelvises. One doctor, John Diamond, MD, actually saw this a long time ago. Here is his assessment of the importance of the palatal arch:
“One of the greatest gifts a child can receive from his mother is a well-formed palatal arch. But it is doubtful whether any of us have ever seen a normal arch because it may well be that only primitive man on his so-called primitive diet has a fairly normal arch. With such an arch, the following benefits are conferred:
- There will be minimal occlusal problems.
- Three of the structures with the most to do with centering and balancing the body in space will be free to function normally: the sphenoid bone, the hyoid bone, and the temporomandibular joint.
- There will be an accompanying development of the lateral aspects of the face – especially of the malar and zygoma (cheek) bones.
- Normal development and stimulation of the pituitary will be facilitated (master hormonal gland).
- The overall health and well-being of the patient will be sound.”[23]
Dr. Diamond concluded by saying: “Maternal nutrition, proper infant feeding and the ability to smile are three of the most important essentials for good health and they all relate to the palatal arch.”
We need to grow larger, “paleo-sized” palates and develop better jaw and tongue function. As Sir William Osler said, “The mouth is the mirror of all disease.” We should all support the simple concept of promoting children’s health through breastfeeding, good nutrition, and trace mineral supplementation. These three practices should be recognized as the birthright of all children globally. This would result in “Paleo-Modern” children with well-formed palates, stronger teeth, better airways, wider pelvises, greater resistance to disease, and overall better mental and physical development. Let us do something powerful together by leaving the next generation a positive legacy from our accumulated knowledge and clinical experience.
Clinical pattern recognition and intuitive clinical interpretation are key elements in medical diagnosis and decision making. However, maxillary dysmorphogenesis and the resulting whole body-mind dysfunctionality are being overlooked. It is time for the world of medicine to recognize maxillary dysmorphogenesis, interpret it correctly, and take action to reverse this significant pathological trend in humanity. An underdeveloped maxilla is, indeed, the canary in the cranium. We must correct this significant growth disorder with a Paleo-Modern strategy and expansion airway-development orthodontics.
About the Author
 George Paul Greenacre, DDS, has been a dental editor for nine of his 49 years of clinical practice and has achieved five dental fellowships, as well as manual osteopath status. He has created over 80 continuing education programs. He writes, consults, and plays four games of hockey per week. Dr. Greenacre is in private practice in Ottawa, Canada, and can be contacted at [email protected].
George Paul Greenacre, DDS, has been a dental editor for nine of his 49 years of clinical practice and has achieved five dental fellowships, as well as manual osteopath status. He has created over 80 continuing education programs. He writes, consults, and plays four games of hockey per week. Dr. Greenacre is in private practice in Ottawa, Canada, and can be contacted at [email protected].
REFERENCES
- Uhlemeyer HA. The chewing mechanism – the body computer. Basal Facts. 1985; 7(1):95-97.
- Schellhas KP, Pollei SR, Wilkes CH. Pediatric internal derangements of the temporomandibular joint: effect on facial development. Am J Orthod Dentofacial Orthop. 1993; 104(1):51-59.
- Olmos SR, Kritz-Silverstein D, Halligan W, Silverstein ST. The effect of condyle fossa relationships on head posture. Cranio. 2005; 23(1):48-52.
- Huang YS, Guilleminault C. Pediatric obstructive sleep apnea and the critical role of oral-facial growth: evidences. Front Neurol. 2013; 3:184. doi: 10.3389/fneur.2012.00184.
- Guilleminault C, Sullivan SS, Huang YS. Sleep-disordered breathing, orofacial growth, and prevention of obstructive sleep apnea. Sleep Med Clin. 2019; 14(1):13-20.
- Hornsby S. ADHD and Orthodontics: Three Things Parents Should Know: An Interview with Dr. Derek Mahony. Youtube. https://www.youtube.com/watch?v=yDHdo4ezs64. Published September 12, 2020.
- Hang W. Seminar at: Capital Dental Symposium, Ottawa, Canada, February 2, 2018.
- Delice M, Gurbuz O, Oflezer C, et al. Palate size and shape in schizophrenia. Psychiatry Res. 2016; 244:273-78.
- Waddington JL, Katina S, O’Tuathaigh CMP, Bowman AW. Translational genetic modelling of 3D craniofacial dysmorphology: elaborating the facial phenotype of neurodevelopmental disorders through the “prism” of schizophrenia. Curr Behav Neurosci Rep. 2017; 4(4):322-30.
- Buckley PF, Dean D, Bookstein FL, et al. A three-dimensional morphometric study of craniofacial shape in schizophrenia. Am J Psychiatry. 2005; 162(3):606-68.
- Leake J. Scientists show we’ve been losing face for 10,000 years. The Sunday Times (UK). November 20, 2005. https://www.thetimes.co.uk/article/scientists-show-weve-been-losing-face-for-10000-years-tgjvhsdd3g7.
- Corriher CT, Corriher SG. Defy Your Doctor and Be Healed. Mocksville, NC: Health Wyze Media; 2013.
- Thompson R, Barnes K. The Calcium Lie II: What Your Doctor Still Doesn’t Know. Take Charge Books; 2013.
- American Academy of Family Physicians. Breastfeeding (Policy Statement). https://www.aafp.org/about/policies/all/breastfeeding.html. Accessed August 26, 2019.
- Academy of Breastfeeding Medicine. About ABM. https://www.bfmed.org/about. Accessed February 11, 2020.
- Swanson NL, Leu A, Abrahamson J, Wallet B. Genetically engineered crops, glyphosate and the deterioration of health in the United States of America. J Organic Syst. 2014; 9(2):6-37.
- Blaylock RL. Food additive excitotoxins and degenerative brain disorders. Medical Sentinel. 1999; 4(6):212-15.
- University of California Television. Sugar: The Bitter Truth with Robert Lustig. Youtube. https://www.youtube.com/watch?v=dBnniua6-oM. Published July 30, 2009.
- Kuroda T, Ono T. Diagnosis and management of oral dysfunction. World J Orthodontics. 2000; 1(2):125-35.
- Cong X, Xu W, Romisher R, et al. Gut microbiome and infant health: brain-gut-microbiota axis and host genetic factors. Yale J Biol Med. 2016; 89(3):299-308.
- James GA. Etiology of malocclusion: contributory factors. Oral Health. March 1, 2018. https://www.oralhealthgroup.com/features/etiology-malocclusion-contributory-factors.
- Price WA. Nutrition and Physical Degeneration (8th ed). Lemon Grove, CA: Price-Pottenger; 2016:380.
- Diamond J. The palatal arch. Basal Facts. 1985; 7(1):55-61.
Published in the Price-Pottenger Journal of Health & Healing
Winter 2019 – 2020 | Volume 43, Number 3
Copyright © 2019 Price-Pottenger Nutrition Foundation, Inc.®
All Rights Reserved Worldwide




