
Access to all articles, new health classes, discounts in our store, and more!
The Low-FODMAP Diet for Relief of IBS and Other Digestive Disorders

Irritable bowel syndrome (IBS) is a functional gastrointestinal disorder that affects between 25 and 45 million Americans.[1] Symptoms can include debilitating abdominal pain and other digestive problems that can seriously impact quality of life. While dietary changes have long been included in strategies to manage symptoms, determining an individual’s specific trigger foods has generally come down to trial and error, and many people have failed to find relief.
Today, mounting evidence suggests that, for many IBS sufferers, symptoms are triggered by a group of carbohydrates known as FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols). But, although up to 86 percent of those suffering with this syndrome may find their symptoms relieved by undertaking a low-FODMAP diet,[2] many people have never even heard of the term.
“FOD-what?” was the general response I received from friends when I mentioned that I was writing this article. Yet, extensive research points to dietary FODMAP reduction as a significant treatment protocol that can benefit millions of people with IBS, and likely other digestive complaints as well. So, what exactly makes these carbohydrates different from others, and why are they causing problems for so many people?
As a general group, FODMAPs are hard-to-digest, short-chain carbohydrates (sugars and fibers) that can trigger abdominal pain, flatulence, diarrhea, constipation, abdominal distension, and bloating – the symptoms typically suffered by those with IBS. These carbohydrates occur naturally in a wide variety of foods and are sometimes used as additives in processed foods.
Unlike many dietary sugars that are easily absorbed in the small intestine, FODMAPs are absorbed slowly or not at all. Poorly digested FODMAPs arrive intact in the large intestine, where they are fermented by our gut bacteria. Like dietary fiber, which is made up of long-chain molecules, they are used as fuel by these bacteria rather than directly feeding our bodies. However, they ferment much more quickly and easily than fiber, resulting in the production of copious amounts of gas, including carbon dioxide, hydrogen, and methane. The fermentation of these carbohydrates also produces short-chain fatty acids. These are normally beneficial, since they are used as fuel by intestinal cells. However, they can speed up the motility of the large intestine and, when produced in excess, can injure the colon wall.
In addition, due to their small molecular size, FODMAPs draw water into the small intestine via osmosis, and this excess water travels to the colon. The increase in water – in addition to the gas produced by fermentation – stretches the intestinal wall, which can lead to bloating, cramping, abdominal distension, and changes in bowel habits (diarrhea and/or constipation).
In some people, FODMAPs can also trigger symptoms that are not always recognized as connected to digestion, such as fatigue, lethargy, and brain fog. Moreover, anxiety and depression are often experienced by those with IBS, and reducing FODMAPs can help to minimize those conditions.
FODMAPs don’t cause problematic symptoms in everyone. Many people can tolerate them with no noticeable effects or with just a minor increase in intestinal gas. However, those plagued with IBS may have more extreme reactions for a variety of reasons, which can include visceral hypersensitivity – an increased sensitivity of the nerves that carry messages from the gut to the brain – and differences in the types of bacteria present in the intestines. In people who are sensitive to FODMAPs, their impacts on health and lifestyle can be devastating – and the benefits of reducing them can be profound.
Who can benefit from reducing FODMAPs?
Growing numbers of doctors and other healthcare practitioners are prescribing a low-FODMAP diet to their patients with IBS, with remarkable results. In fact, the diet is now considered a first-line therapy for the disorder in many parts of the world. In addition, those with IBS-like symptoms but no clinical diagnosis may benefit from the diet.
The vast majority of research relating to FODMAPs has been centered on IBS. However, reducing them can be beneficial to people with other gastrointestinal problems as well. People with inflammatory bowel disease or small-intestinal bacterial overgrowth (SIBO) may find that a low-FODMAP diet helps them to manage their IBS-like symptoms. Those with gastroesophageal reflux disease (GERD) may also benefit from reducing FODMAPs, particularly fructans (see the description of oligosaccharides, below).
This brings us to a brief discussion of FODMAPs and gluten. Many IBS sufferers find that wheat and other gluten-containing grains trigger their symptoms, and some of them have turned to a gluten-free diet, with mixed results. However, for many of these individuals, gluten – a group of related proteins in wheat, barley, and rye – may not actually be the problem. The trigger may instead be fructans, which are found in high amounts in cereal grains.
Similarly, many people who believe they have non-celiac gluten sensitivity because eliminating wheat and other gluten grains resolves their IBS-like symptoms may actually be sensitive to FODMAPs, rather than gluten. Due to its omnipresence in modern foods, wheat is a major contributor of fructans in the standard American diet. Because the effects of various FODMAPs eaten at the same time are cumulative, and symptoms may only arise after a certain threshold is reached, a significant reduction in the intake of one major source may reduce or even resolve symptoms. If giving up gluten – or dairy, another source of FODMAPs – reduces one’s gastrointestinal symptoms but does not fully resolve them, there’s a good chance FODMAPs may be the culprit.
Types of FODMAPs
There are several categories of FODMAPs, each of which functions somewhat differently within the human body:
Oligosaccharides (oligo means “few,” and saccharides means “sugars”) are composed of three to ten simple sugars linked together. This group includes two types of carbohydrates: fructans and galacto-oligosaccharides (GOS). Fructans are found in foods such as wheat, onions, and garlic, and GOS are found in pulses and legumes (e.g., beans, peas, and lentils). These sugars are actually malabsorbed and fermented by everyone, because the human body lacks the enzymes needed to break their molecular bonds. However, many people without gastrointestinal disorders can tolerate them. Although oligosaccharides are believed to encourage the growth of good bacteria in the gut, they can lead to significant functional symptoms in people with IBS.
Disaccharides are formed from two simple sugars. Although sucrose and maltose are also disaccharides, only lactose (composed of the simple sugars galactose and glucose) is a FODMAP. Lactose is found in milk and other dairy products and causes gastrointestinal symptoms in people with lactose intolerance (those who lack sufficient quantities of the enzyme lactase to digest it properly). However, many with lactose intolerance can consume small amounts of it with no ill effect. Thus, some dairy foods that are lower in lactose, such as natural, aged cheddar and swiss cheese, as well as butter, may be tolerated in small portions.
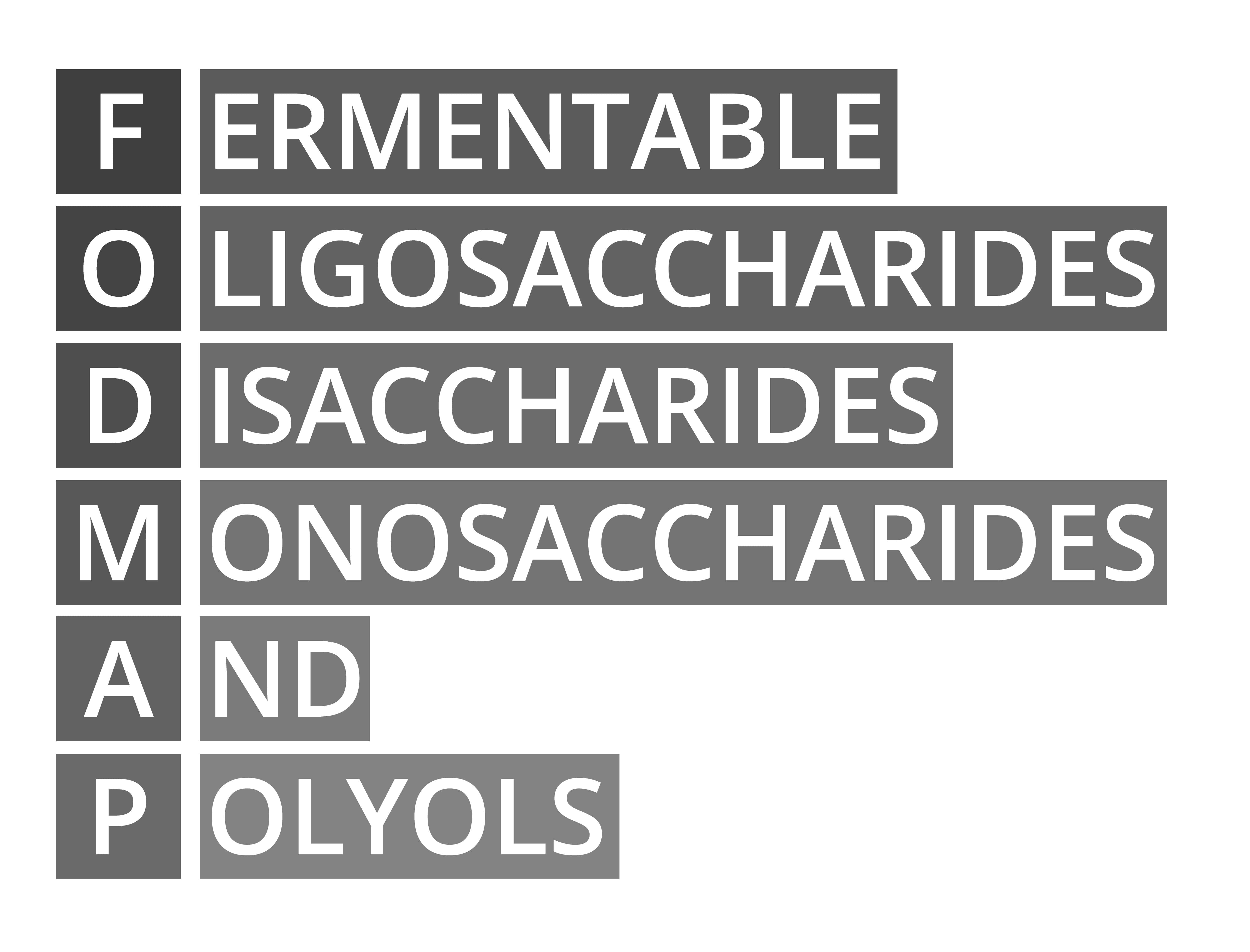
Monosaccharides consist of a single sugar. The only monosaccharide considered to be a FODMAP is fructose, which is found in fruits, vegetables, and various sweeteners. Fructose is not fully absorbed by some people, but it generally causes gastrointestinal difficulties only when it is present in high concentrations (as in fruit juice, agave nectar, or high-fructose corn syrup) or when there is more fructose than glucose – another simple sugar – in a food (as in mangos, figs, or honey). Thus, fruits that contain equal amounts of glucose and fructose (such as bananas) or less fructose than glucose (such as apricots and peaches) are likely to be more easily tolerated.
Polyols (also known as sugar alcohols) include sorbitol, manitol, and xylitol, among others. Polyols are found in some fruits and vegetables and are sometimes added to processed foods or other products as sweeteners. Sorbitol is found in fruits such as pears, cherries, and avocado; and manitol is present in foods such as mushrooms and cauliflower. Xylitol occurs in small amounts in many fruits and vegetables, but when used as an additive in “sugar-free” products, it is generally sourced from either corn cobs or hardwoods, such as birch. In most people, polyols are slowly and incompletely absorbed in the small intestine.
As the above introduction suggests, most foods – even healthy ones – contain some amount of FODMAPs, with the exception of fats and animal-based proteins, and a small handful of fruits and vegetables that have not shown any detectable FODMAP content. A diet that completely excluded all these foods would be extremely limiting. Not only would it be impossible to maintain for the general population, it would pave the way for nutrient deficiencies.
Thus, the low-FODMAP diet is not like the gluten-free diet, which eliminates all traces of gluten. The therapeutic benefits of reducing FODMAP consumption are instead gained through the use of a personalized low-FODMAP diet, which includes as many different foods as are tolerated. Individuals may be sensitive to certain categories of FODMAPs, or to specific foods within those categories, or only to quantities of those foods that exceed certain thresholds. A person’s level of sensitivity may also be influenced by the total amount of FODMAPs consumed during the same meal. Attention must therefore be paid to portion sizes. Moreover, one’s sensitivities to specific foods may change over time, allowing the reintroduction of foods that previously caused problems. Thus, undertaking a low-FODMAP diet can be a bit complicated and will generally be achieved most effectively under the guidance of a knowledgeable healthcare practitioner.
The low-FODMAP diet
The low-FODMAP diet was first created by researchers at Monash University in Melbourne, Australia, more than a decade ago, and it is continually being refined as testing is conducted on additional foods. Its basic aim is to help people with IBS overcome their symptoms and design a personalized diet that enables them to reduce or eliminate their trigger foods while maximizing the range of healthy foods they consume.
To this end, the diet has three phases: an initial elimination diet, in which all high-FODMAP foods are restricted to calm the digestive tract; a series of challenges, in which foods are individually reintroduced to identify the individual’s specific triggers; and an integration and maintenance period, in which the tolerated foods (and perhaps some trigger foods in tolerated amounts) are reincorporated into the diet.
Elimination Phase
In the first phase, high-FODMAP foods should be eliminated from the diet for a period of two to six weeks, or until symptoms have abated. If FODMAPs are indeed a problem for you, you will likely begin to see a lessening of symptoms within the first week or two. Although allowable foods are drawn from a range of categories – including low-FODMAP vegetables, fruits, and grains; animal proteins; fats; some nuts and seeds; and even certain sweeteners – the elimination diet is quite restrictive and is not intended to be maintained over the long term.
Challenge Phase
This phase is designed to reveal which FODMAPs you can tolerate and which are problematic for you. The exact protocol for conducting these challenges may vary slightly under the guidance of different healthcare practitioners. In general, it will involve undertaking a different FODMAP challenge every week or so, recording any symptoms in a journal or log, and then eliminating that category of food from the diet again in order to return to a baseline level before beginning the next test.
Here are some general guidelines: Only one FODMAP subtype (lactose, excess fructose, fructans, GOS, or polyols) should be tested at a time, and the food chosen to represent it should not contain any of the other subtypes. That food should be consumed once a day, in increasing doses, three times during the given week. If symptoms arise, immediately stop the challenge, write down the symptoms, and wait at least three days after they subside before beginning the next challenge. If there is no reaction, another subtype may be tested at the week’s end, after you discontinue the food you just challenged. Sometimes, you may choose to retest specific subtypes that provoked symptoms, using smaller doses. After you have completed all the individual subtype challenges, you can try some additional challenges with foods containing multiple subtypes.
If a healthcare practitioner is facilitating your diet, they will help you select foods and portion sizes for the individual challenges. If you decide to undertake the challenges on your own, books such as The Low-FODMAP Diet Step by Step (see the Resources section at the end of this article) can provide specific guidance. This phase can take six to eight weeks, but, in the end, you will have a good idea of what foods you can tolerate.
Integration Phase
After you have completed the challenges, the foods that were well tolerated should be slowly reincorporated into the diet, and those that were moderately well tolerated may be reintroduced on an occasional basis. The goal, as previously stated, is to maintain as varied a diet as possible without causing symptoms to return. For this reason, over time, people are encouraged to do additional challenges with eliminated foods to see whether their sensitivity to those foods has decreased.
Remember that tolerance can be dose-dependent and that the total amount of various subtypes of FODMAPs consumed at a meal may affect your sensitivity to the individual components of the meal. Thus, portion control can be a significant factor in remaining symptom-free. If symptoms do flare, you can always return to the elimination diet for a couple of days until they subside.
Dietary cautions
It is important when reducing FODMAPs to make sure the diet remains nutritionally adequate. Over-restricting FODMAPs can lead to insufficient intake of nutrients, such as calcium, B vitamins, and fiber. Vegetarians and vegans will face additional challenges, as many common vegetable-based protein sources are high in FODMAPs, and attention will be required to ensure adequate intake of vitamin B12, iron, and zinc.

With children, it is particularly important to make sure they are getting enough nutrients and to not restrict the diet more than is necessary. They should be rechallenged with eliminated foods regularly, with the aim of adding back any that become tolerated. Be aware that young children have a lower capacity to absorb fructose, and that their tolerance for fructose-containing foods may increase as they get older.
For people who are accustomed to eating wheat, removing it from the diet may cause fiber intake to drop significantly. As adequate amounts of fiber are important for gut health, other sources, such as oats, quinoa, chia and pumpkin seeds, oranges, and raspberries, should be consumed. Proper hydration is also necessary to help move that fiber through the intestine.
A very low-FODMAP diet in which fructans and GOS are highly restricted may lead to changes in the gut microbiota. These carbohydrates are prebiotic; in other words, they feed our beneficial bacteria. A couple of short-term studies showed an association between implementation of a very low-FODMAP diet and a reduction in the number of Bifidobacteria in the feces, and in one study, a low-FODMAP diet reduced overall bacterial abundance.[3,4] However, in a large trial, the administration of probiotics was able to mitigate some of the changes to the microbiota. Future studies are needed to determine the long-term effect of such a diet on the gut microbiome.
Food choices
Even in the elimination phase of the low-FODMAP diet, there are enough food options available to provide diversity – and flavor – in one’s meals. The challenge is to determine which foods meet the dietary guidelines, and in what quantities. Fortunately, there are a variety of informative books and websites that provide lists of foods with high-, medium-, and low-FODMAP content. (See the Resources section for a few examples.) Many of these sources also include portion sizes that should not be exceeded, as well as recipes and meal plans.

The most accurate and up-to-date information on the FODMAP content of food will come directly from Monash University, where ongoing research is being conducted to expand the comprehensive food database. At the Monash lab, each food is individually analyzed in a process that can take two to four weeks, after which a dietician determines portion sizes that would be considered low, moderate, or high FODMAP. This information is available to consumers through the Monash University FODMAP Diet app, which can be downloaded from www.monashfodmap.com. Note, however, that the FODMAP content of fruits and vegetables is somewhat variable, depending on factors that include the season in which they were grown and their maturity when picked.
The following section provides examples of high- and low-FODMAP foods. This list is not broken down by subtype and will not be sufficient to guide the reader in undertaking a low-FODMAP diet. Rather, it is intended to indicate the extent of the diet and to show some of the alternatives to restricted foods. Remember that FODMAP toleration is often dose-dependent, so strict attention to portion size is necessary.
Meat, seafood, and eggs
High-FODMAP: Dishes prepared with high-FODMAP seasonings, such as garlic or onions
Low-FODMAP: Plain cooked meat, poultry, seafood, and eggs
Note: Because FODMAPs are carbohydrates, no animal proteins are restricted on this diet.
Dairy products
High-FODMAP: Milk and yogurt from cows, goats, and sheep; some soft cheeses, such as cottage, ricotta, and mascarpone
Low-FODMAP: Butter, ghee, and some cheeses, such as cheddar, swiss, brie, blue, feta, and parmesan; all lactose-free dairy products
Note: In general, aged and hard cheeses tend to have less lactose than softer ones. However, for most people, even the high-lactose dairy products will be tolerated if consumed in sufficiently small quantities, such as a spoonful or two of soft cheese or yogurt, or a splash of milk in tea or coffee.
Grains
High-FODMAP: Wheat, barley, rye
Low-FODMAP: Buckwheat, millet, oats, quinoa, rice, corn, tapioca, teff
Note: For many people with IBS, wheat and other high-FODMAP cereal grains may be tolerated if present in small quantities as food ingredients.
Legumes
High-FODMAP: Beans (red, navy, black, butter), dried chickpeas and lentils, split peas, soybeans
Low-FODMAP: Canned chickpeas and lentils (drained and rinsed)
Note: Although legumes are naturally high in GOS and fructans, these oligosaccharides are water soluble and their amounts will vary based on cooking and processing methods. When legumes are canned or boiled, some proportion of the oligosaccharides leaches out into the canning/cooking water and will be removed when the legumes are drained and rinsed.
Also, mature soybeans are high in FODMAPs, but young edamame beans are not. In addition, the FODMAP content is reduced in the manufacture of some soy products, such as miso, tempeh, and firm tofu, so those foods may be tolerated in limited amounts.
Vegetables
High-FODMAP: Artichokes, asparagus, cauliflower, sugar snap peas, mushrooms, garlic, onions, leeks
Low-FODMAP: Arugula, bell peppers, bok choy, broccoli, carrots, kale, spinach, green beans, potatoes, zucchini, eggplant, ginger root
Note: Due to their highly concentrated fructan content, onion and garlic (including powdered forms) generally need to be strictly eliminated on a low-FODMAP diet, unless the challenge phase reveals that they are well tolerated. Olive oil infused with onion or garlic may be used as a replacement, as fructans are not oil soluble. The green parts of spring onions and chives are also a good onion substitute.
Fruit
High-FODMAP: Apples, cherries, mangos, pears, watermelon, nectarines, blackberries, plums, peaches
Low-FODMAP: Bananas, lemons, limes, oranges, blueberries, strawberries, raspberries, cantaloupe, coconut, grapes, pineapple
Note: Due to the high sugar content of fruit, limiting even low-FODMAP fruit to one serving per meal is recommended.
Nuts and seeds
High-FODMAP: Cashews, pistachios
Low-FODMAP: Almonds, macadamias, walnuts, Brazil nuts, peanuts; sunflower, sesame, and pumpkin seeds
Note: Activating nuts (soaking them in water and salt until they germinate and then dehydrating them) can lower their FODMAP content.
Sweeteners
High-FODMAP: Honey, molasses, agave nectar, high-fructose corn syrup
Low-FODMAP: Maple syrup, rice malt syrup, stevia
Note: Sugar (sucrose) and artificial sweeteners are also low-FODMAP but should be avoided for other health reasons.
Beverages
High-FODMAP: Fruit juice and cider, soy milk, some teas (fennel, chamomile, oolong)
Low-FODMAP: Almond, coconut, hemp, and oat milks; black, green, and white teas; most herbal teas
Closing thoughts
While the causes of IBS are not completely understood, it is known that a variety of factors can contribute to its development. These can include genetic predisposition, previous bacterial infection in the digestive tract, and chronic stress or anxiety. Thus, it would stand to reason that the best treatment should be multifactorial as well. To truly heal from any chronic health condition, the individual must be considered as whole, and all imbalances must be addressed. In addition to dietary changes, such lifestyle modifications as developing healthy sleep habits, practicing stress reduction techniques, and maintaining an appropriate exercise program are likely to prove beneficial.
However, removing trigger foods that provoke debilitating symptoms is a critical step in healing from IBS and similar gastrointestinal conditions. For many people, this alone may bring about symptom resolution. For others, it may bring sufficient relief to allow for the beginning of a more wide-ranging healing journey. Either way, the low-FODMAP diet has been shown to be an invaluable tool, relieving symptoms for the majority of IBS sufferers who undertake it. For those whose lives are compromised by the pain and discomfort of IBS, it certainly seems well worth the effort.
About the Author

Roberta Louis is managing editor of the Price-Pottenger Journal, a contributing editor at Well Being Journal, and founder of the Shaman’s Drum Foundation. She is a freelance writer and editor specializing in complementary and alternative healing methods. She may be contacted at: [email protected].
REFERENCES
International Foundation for Gastrointestinal Disorders. Facts About IBS. Available at: https://www.aboutibs.org/facts-about-ibs.html. Accessed December 27, 2018.
Nanayakkara WS, Skidmore PML, O’Brien L, et al. Efficacy of the low FODMAP diet for treating irritable bowel syndrome: the evidence to date. Clin Exp Gastroenterol. 2016; 9:131-42.
Hill P, Muir JG, Gibson, PR. Controversies and recent developments of the low-FODMAP diet. Gastroenterol Hepatol. 2017; 13(1):36-45.
Whelan K, Martin LD, Staudacher HM, Lomer MCE. The low FODMAP diet in the management of irritable bowel syndrome: an evidence-based review of FODMAP restriction, reintroduction, and personalisation in clinical practice. J Hum Nutr Diet. 2018; 31:239-255.
Resources / Recommended Reading
Monash University. The Low FODMAP Diet website. www.monashfodmap.com (includes download for smartphone app).
The Low-FODMAP Diet Step by Step by Kate Scarlata and Dédé Wilson. New York, NY: Da Capo Press; 2018. Informational website at: katescarlata.com (includes low- and high-FODMAP food checklists).
The 2-Step Low-FODMAP Eating Plan by Sue Shepherd. New York, NY: The Experiment; 2016. shepherdworks.com.au.
World Gastroenterology Organisation. WGO Practice Guideline – Diet and the Gut. April 2018. worldgastroenterology.org/guidelines/global-guidelines/diet-and-the-gut.
Published in the Price-Pottenger Journal of Health & Healing
Fall 2018 | Volume 42, Number 3
Copyright © 2018 Price-Pottenger Nutrition Foundation, Inc.®
All Rights Reserved Worldwide




